A 52-year-old woman from Mumbai presents with a 6-month history of progressive weakness in thumb opposition and flexion of the index and middle fingers at the interphalangeal joints. She denies sensory complaints. Examination reveals weakness of flexor pollicis longus, flexor digitorum superficialis (index and middle), and pronator teres. Wrist flexion is weak. There is no thenar eminence atrophy. Which segment of the median nerve is most likely affected?
A. Median nerve proximal to the pronator teres
B. Recurrent motor branch at the carpal tunnel
C. Anterior interosseous nerve (AIN) branch
D. Median nerve distal to the carpal tunnel
Explanation
Clinical Diagnosis: Proximal Median Nerve Lesion
Motor Anatomy of the Median Nerve
Key Point
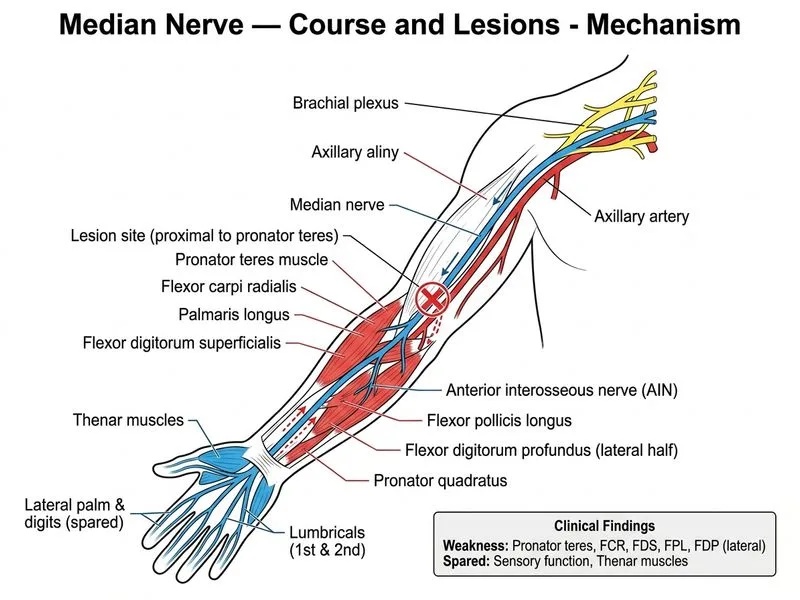
The median nerve gives off motor branches at three key levels: (1) proximal to pronator teres (flexor carpi radialis, palmaris longus, flexor digitorum superficialis), (2) at/through pronator teres (pronator teres itself), and (3) as the anterior interosseous nerve (AIN) distal to pronator teres (flexor pollicis longus, flexor digitorum profundus index, pronator quadratus).
This patient's motor deficit pattern indicates a lesion proximal to the pronator teres:
Motor Deficit Analysis
Table
Muscle
Innervation
Status in Case
Interpretation
Pronator teres
Median nerve at level of pronator
Weak
Lesion at or proximal to pronator teres
Flexor carpi radialis
Median nerve proximal to pronator
Weak (implied)
Confirms proximal lesion
Palmaris longus
Median nerve proximal to pronator
Weak (implied)
Confirms proximal lesion
Flexor digitorum superficialis
Median nerve proximal to pronator
Weak
Confirms proximal lesion
Flexor pollicis longus
AIN (distal to pronator)
Weak
Lesion extends distally through pronator
Flexor digitorum profundus (index)
AIN (distal to pronator)
Weak (implied)
Lesion extends distally through pronator
Thenar eminence (APB, opponens)
Recurrent motor branch (distal to carpal tunnel)
Normal
Recurrent branch is spared; lesion is proximal
High-YieldNEET PG
The preservation of thenar eminence function (no atrophy) is the critical distinguishing feature. This rules out carpal tunnel syndrome (which affects the recurrent motor branch) and indicates a proximal lesion that affects pronator teres and flexor digitorum superficialis but spares the distal recurrent branch.
Why Each Level Is Ruled Out
Loading diagram...
Clinical Pearl
Clinical Pearl
Proximal median nerve lesions (e.g., from supracondylar fracture, brachial plexus injury, or compression at the ligament of Struthers) present with a characteristic pattern: weakness of pronator teres, flexor carpi radialis, palmaris longus, and flexor digitorum superficialis, plus AIN syndrome features (weak FPL and FDP index). The absence of thenar atrophy distinguishes this from carpal tunnel syndrome.
Mnemonic for Median Nerve Motor Branches (Proximal to Distal)