This patient presents with severe carpal tunnel syndrome (CTS) — the most common entrapment neuropathy of the median nerve. The clinical findings include:
This constellation — particularly the thenar atrophy and distal motor latency >6.0 ms — classifies this as severe CTS, not mild-to-moderate disease.
| Severity | DML | Clinical Features | Management |
|---|---|---|---|
| Mild | <4.5 ms | Sensory symptoms only | Conservative |
| Moderate | 4.5–6.0 ms | Sensory + mild motor | Conservative → Surgery if failed |
| Severe | >6.0 ms | Thenar atrophy, motor weakness | Surgical decompression |
Conservative management (wrist splinting + NSAIDs) is inappropriate here — thenar atrophy and DML >6.0 ms indicate severe, established disease. Conservative measures cannot reverse denervation and delay definitive treatment, risking permanent motor loss.
EMG is unnecessary — NCS already confirms the diagnosis and severity (DML 6.2 ms). EMG would add information about denervation but would not change the management decision in a patient with overt thenar atrophy.
MRI of the wrist is not indicated — there is no clinical suspicion of a space-occupying lesion, trauma, or atypical presentation. MRI would delay necessary surgical intervention without adding diagnostic value.
In a patient with thenar atrophy + DML >6.0 ms, the most appropriate next step is immediate carpal tunnel release, which has a 70–90% success rate in halting progression and improving motor function when performed before complete axonal degeneration.
Loading illustration…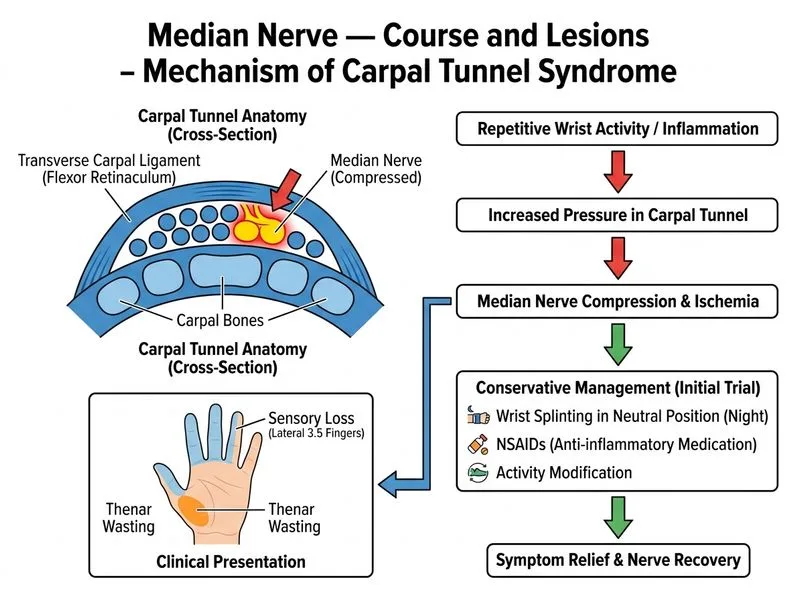
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →