Median Nerve — Course and Lesions MCQ — NEET PG Practice Question | NEETPGAI
Median Nerve — Course and Lesions
hard
bone Anatomy
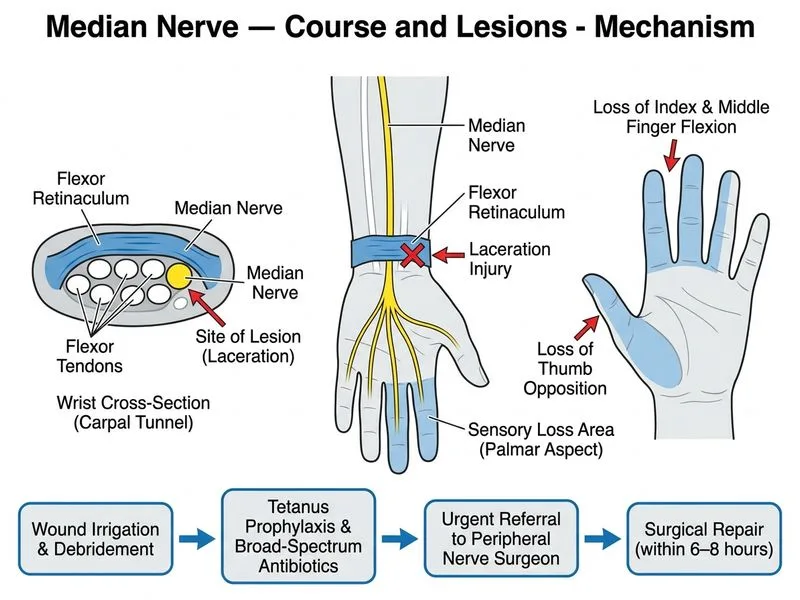
A 28-year-old male from Mumbai sustained a laceration to the volar aspect of the wrist during a knife injury 6 hours ago. Clinical examination reveals loss of thumb opposition and flexion of the index and middle finger interphalangeal joints, with sensory loss in the thumb, index, middle, and lateral half of the ring finger. The wound is contaminated. What is the most appropriate immediate next step in management?
A. Immediate primary repair of the median nerve under operating microscope after wound debridement and irrigation
B. Conservative dressing with observation for 2 weeks to allow inflammation to settle before nerve repair
C. Wound irrigation, tetanus prophylaxis, broad-spectrum antibiotics, and urgent referral to a peripheral nerve surgeon for assessment and repair within 6–8 hours
D. Electromyography to confirm the level and extent of median nerve injury before surgical planning
Explanation
Clinical Scenario Analysis
This patient has a complete acute median nerve transection at the wrist level, evidenced by:
Loss of thumb opposition (Opponens pollicis — recurrent motor branch of median nerve)
Loss of flexion of index and middle finger DIP joints (Flexor digitorum profundus to digits 2–3 — anterior interosseous nerve, a branch of median nerve)
Sensory loss in the distribution of median nerve (thumb, index, middle, lateral ring finger)
Acute mechanism (knife laceration) with contaminated wound
Immediate Management Priorities
Loading diagram...
Why NOT Immediate Primary Repair?
High-YieldNEET PG
Although the golden period for nerve repair is 6–12 hours, a contaminated wound takes priority. Attempting primary repair in a contaminated field risks:
Infection control first — irrigation, debridement, antibiotics, tetanus prophylaxis
2.
Urgent specialist referral — peripheral nerve surgeon or hand surgeon
3.
Delayed primary or secondary repair — once infection risk is minimized (typically 24–72 hours)
Clinical Pearl
In contaminated wounds, delayed primary repair (within 3 weeks) has outcomes nearly equivalent to immediate primary repair, but with far lower infection morbidity. The nerve ends can be tagged with a suture to prevent retraction if time permits.
Correct Management Sequence
1.
Immediate (at presentation):
Hemostasis and elevation
Copious irrigation with normal saline
Tetanus prophylaxis (if indicated)
Broad-spectrum antibiotics (e.g., amoxicillin-clavulanate + gentamicin for contaminated wounds)
Dressing with sterile, non-adherent material
2.
Urgent (within 6–8 hours):
Referral to peripheral nerve surgeon or hand surgeon
Assessment of wound, nerve, and surrounding structures
Decision on timing of repair (delayed primary vs. secondary)
3.
Surgical (24–72 hours):
Formal debridement under anesthesia
Nerve repair under operating microscope (if infection risk controlled)
Tension-free, epineurial or fascicular repair
Why NOT the Other Options?
Immediate primary repair without infection control is dangerous — the contaminated wound is a contraindication to immediate repair. Infection will compromise the repair and may lead to permanent disability or amputation.
Conservative dressing with observation for 2 weeks is inappropriate — the nerve ends will retract and become scarred, making later repair technically difficult or impossible. The patient will have progressive denervation atrophy during this period.
EMG at this stage is premature and unnecessary — the clinical diagnosis is clear. EMG is useful for prognostication or detecting partial injuries, but it should not delay urgent surgical referral. EMG is typically done at 2–3 weeks post-injury to assess for denervation.
Prognosis
With appropriate delayed primary repair, recovery of median nerve function is good — sensory recovery is often excellent, and motor recovery (thumb opposition) is fair to good if repair is performed within 3 weeks.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.