A 58-year-old vegetarian woman from rural India presents with progressive fatigue, dyspnea on exertion, and paresthesias in both feet for 3 months. On examination, she has glossitis, angular cheilitis, and a positive Romberg test. Blood investigations show hemoglobin 7.2 g/dL, MCV 118 fL, and reticulocyte count 0.8%. Peripheral blood smear reveals hypersegmented neutrophils and macro-ovalocytes. Serum vitamin B12 level is 95 pg/mL (normal >200). What is the most likely diagnosis?
A. Megaloblastic anemia due to vitamin B12 deficiency
B. Macrocytic anemia due to hypothyroidism
C. Sideroblastic anemia with neurological manifestations
D. Megaloblastic anemia due to folate deficiency
Explanation
Clinical Diagnosis
Key Point
This patient has megaloblastic anemia with confirmed vitamin B12 deficiency (serum B12 95 pg/mL) and neurological manifestations (paresthesias, positive Romberg test) pathognomonic for B12 deficiency.
Diagnostic Features
Table
Feature
Finding
Significance
MCV
118 fL
Macrocytic (>100 fL)
Peripheral smear
Hypersegmented neutrophils, macro-ovalocytes
Megaloblastic pattern
Serum B12
95 pg/mL
Frankly low (<200 pg/mL)
Neurological signs
Paresthesias, positive Romberg
B12-specific (not seen in folate deficiency)
Reticulocyte count
0.8%
Inappropriately low for degree of anemia
Dietary history
Vegetarian
Risk factor for B12 deficiency
Pathophysiology of B12 Deficiency Anemia
1.
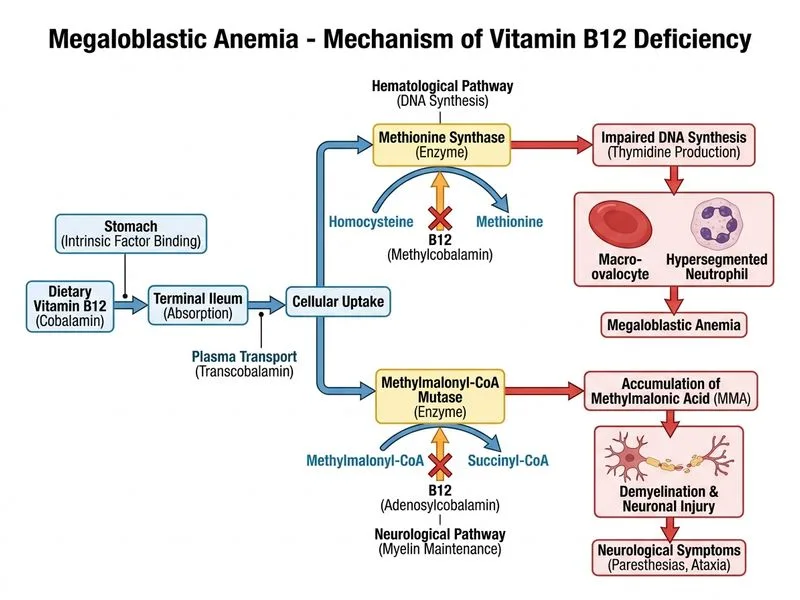
DNA synthesis impairment: B12 (as methylcobalamin) is essential for methionine synthase, which converts homocysteine to methionine. Without adequate B12, deoxyribonucleotide synthesis fails.
2.
Nuclear-cytoplasmic asynchrony: Cytoplasm matures normally while nuclear maturation lags, producing large cells with immature chromatin pattern (megaloblasts).
Neurological manifestations (paresthesias, ataxia, positive Romberg) are SPECIFIC to B12 deficiency and do NOT occur in folate deficiency alone. This is the key discriminator.
Why B12 Deficiency in This Patient
Vegetarian diet (no animal products = no B12 source)
Serum B12 definitively low (95 pg/mL)
Neurological signs present (folate deficiency does not cause myelopathy)
Hypersegmented neutrophils (classic for megaloblastic anemia)
Clinical Pearl
In India, dietary B12 deficiency is common among vegetarians and vegans. Pernicious anemia (autoimmune) is less common but must be ruled out with intrinsic factor antibodies if dietary intake is adequate.
Management Approach
Loading diagram...
Mnemonic: NEUROLOGICAL B12 — N.E.U.R.O.L.O.G.I.C.A.L = Never Expect Usual Reversibility Of Loss; Only Gradual Improvement; Lasting Axonal damage
Neurological damage can be irreversible if B12 replacement is delayed >6 months.
Early treatment prevents permanent myelopathy.
Robbins 10e Ch 14
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.