Megaloblastic Anemia MCQ — NEET PG Practice Question | NEETPGAI
Megaloblastic Anemia
hard
microscope Pathology
A 42-year-old man with a 10-year history of Crohn's disease presents with progressive weakness and cognitive slowing over 4 months. He reports chronic diarrhea and recent weight loss. Examination reveals glossitis, loss of vibration sense in both lower limbs, and a positive Lhermitte sign. Laboratory findings: hemoglobin 8.5 g/dL, MCV 105 fL, serum B12 95 pg/mL, serum folate 6.2 ng/mL (normal >5.4). Bone marrow shows megaloblastic erythropoiesis with giant metamyelocytes. What is the primary mechanism of anemia in this patient?
A. Impaired intrinsic factor secretion due to gastric involvement
B. Autoimmune destruction of parietal cells
C. Malabsorption of cobalamin in the terminal ileum due to Crohn's disease
D. Nutritional folate deficiency from chronic diarrhea
Explanation
Clinical Context: B12 Deficiency in Crohn's Disease
Key Point
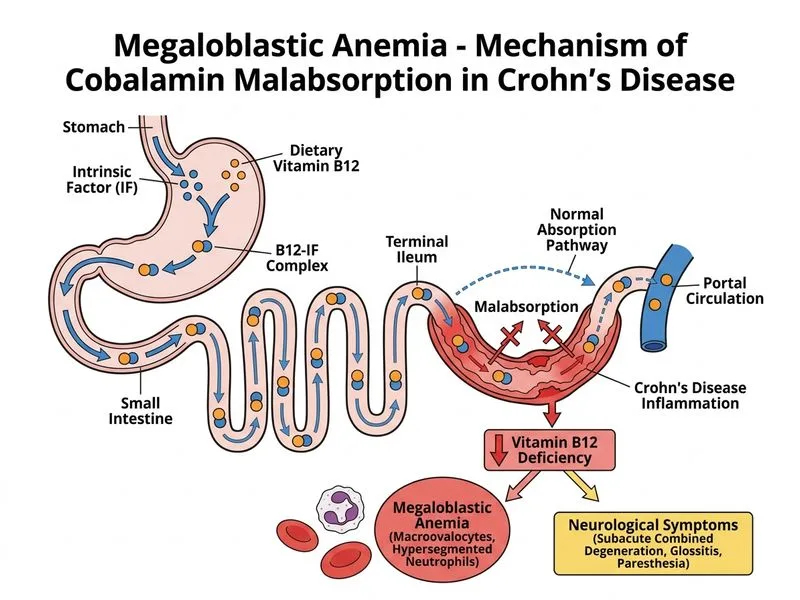
Crohn's disease causes B12 deficiency primarily through malabsorption in the terminal ileum, where the intrinsic factor–B12 complex is absorbed. This is the most common mechanism of B12 deficiency in inflammatory bowel disease.
Why Terminal Ileum Matters for B12 Absorption
Table
Step
Location
Function
Affected in Crohn's?
B12 binding to intrinsic factor
Stomach
Gastric parietal cells secrete IF
No (stomach usually spared)
Transit through small bowel
Duodenum, jejunum
Passive transit
Possibly, if inflamed
Absorption of IF–B12 complex
Terminal ileum
Specific receptor-mediated uptake
YES — primary site of Crohn's involvement
Enterohepatic circulation
Ileum
Reabsorption of B12 from bile
Disrupted in Crohn's
High-YieldNEET PG
Crohn's disease classically affects the terminal ileum (ileitis). This is the site of B12 absorption, making malabsorption the primary mechanism — not intrinsic factor deficiency.
Pathophysiology of B12 Deficiency in IBD
Loading diagram...
Clinical Features Supporting B12 Deficiency
1.
Neurological signs: Loss of vibration sense, positive Lhermitte sign → posterior/lateral column disease (subacute combined degeneration)
2.
Megaloblastic anemia: MCV 105 fL, bone marrow shows megaloblastic erythropoiesis with giant metamyelocytes
3.
Serum B12 frankly low: 95 pg/mL (normal >200)
4.
Serum folate normal: 6.2 ng/mL (>5.4) — rules out pure folate deficiency
5.
Crohn's disease with terminal ileal involvement: Classic risk factor for B12 malabsorption
Clinical Pearl
In Crohn's disease, B12 deficiency is often asymptomatic hematologically but presents with neurological symptoms first (cognitive slowing, paresthesias, ataxia). This is because neurological damage accumulates silently and becomes apparent only when stores are severely depleted.
Why NOT the Other Mechanisms
Intrinsic factor deficiency (pernicious anemia):
Requires autoimmune destruction of gastric parietal cells
Associated with atrophic gastritis, not Crohn's disease
Stomach is rarely involved in Crohn's (usually terminal ileum)
Would require positive intrinsic factor antibodies
Folate deficiency:
Serum folate is normal (6.2 ng/mL)
Folate deficiency causes megaloblastic anemia but NOT neurological manifestations
Crohn's can cause folate malabsorption, but this patient's folate is replete
Parietal cell autoimmunity:
Not associated with Crohn's disease
Would cause pernicious anemia, not Crohn's-related B12 deficiency