A 58-year-old man from Mumbai presents to the emergency department with acute onset chest pain radiating to the left arm for the past 3 hours. He has a history of hypertension and smoking. On examination, blood pressure is 95/60 mmHg, heart rate 110/min, and respiratory rate 24/min. ECG shows ST elevation in leads II, III, and aVF with reciprocal ST depression in I and aVL. Cardiac troponin I is elevated at 2.8 ng/mL (normal <0.04). On coronary angiography, a complete thrombotic occlusion of the right coronary artery is identified. Which of the following pathological changes would be MOST prominent in the myocardium at this 3-hour timepoint?
A. Coagulation necrosis with contraction band necrosis
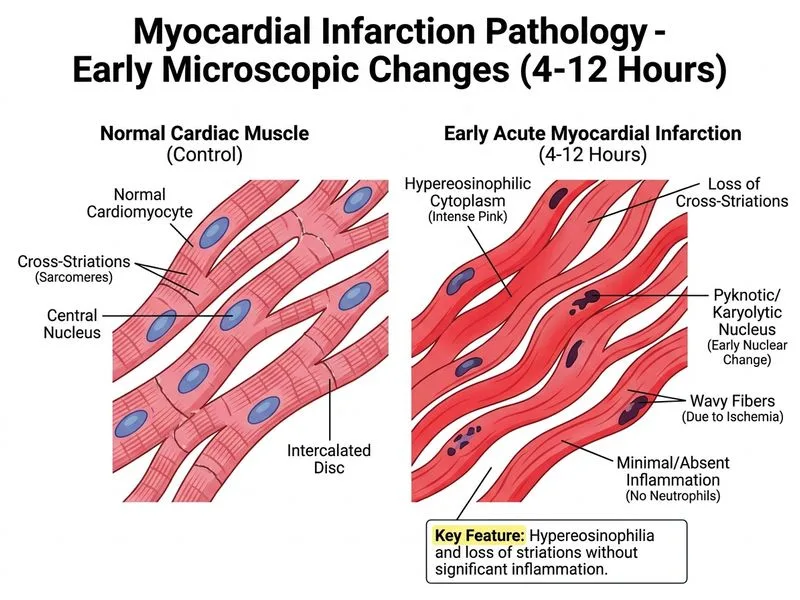
B. Hypereosinophilia and loss of striations without significant inflammation
C. Wavy fibers at the border zone with early neutrophilic infiltration
D. Granulation tissue formation with fibroblast proliferation
Explanation
Temporal Evolution of Myocardial Infarction Pathology
The pathological changes in acute myocardial infarction follow a predictable timeline based on the duration of ischemia and reperfusion status.
Timeline of Histological Changes
Table
Time Since Onset
Pathological Features
Microscopic Appearance
0–4 hours
Hypereosinophilia, loss of striations, wavy fibers at border
No inflammation yet
4–12 hours
Early neutrophilic infiltration begins
Contraction band necrosis appears
12–24 hours
Coagulation necrosis, heavy neutrophil infiltrate
Granular appearance
3–7 days
Macrophage infiltration, granulation tissue
Vascular proliferation
>2 weeks
Fibroblast proliferation, collagen deposition
Scar formation
At 3 Hours Post-Infarction
Key Point
At 3 hours, the myocardium has undergone coagulation necrosis but the light microscopic changes are subtle and non-specific. The cardinal early finding is hypereosinophilia with loss of striations due to protein denaturation and edema, without significant inflammatory cell infiltration.
High-YieldNEET PG
The earliest detectable change on light microscopy is loss of the normal basophilic appearance (due to loss of ribosomes) and increased eosinophilia. Neutrophils do not appear until 4–6 hours post-infarction.
Clinical Pearl
Electron microscopy at 3 hours shows mitochondrial swelling, sarcolemmal disruption, and Z-disc streaming — but these are not visible on routine light microscopy.
Why Other Options Are Incorrect at 3 Hours
Contraction band necrosis develops at 4–12 hours, not at 3 hours. This represents reperfusion injury and is a hallmark of the 4–24 hour window.
Wavy fibers with early neutrophilic infiltration occur at 4–12 hours when inflammation begins; at 3 hours, neutrophils are absent.
Granulation tissue and fibroblast proliferation are late changes (3–7 days), characteristic of the healing/reparative phase.
Mnemonic
HELO — Hypereosinophilia, Early (no inflammation), Loss of striations, Onset (first 4 hours).
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.