A 65-year-old woman with hypertension and diabetes is admitted with acute anterior wall ST-elevation myocardial infarction. She undergoes successful primary percutaneous coronary intervention (PCI) with stent placement. On day 3 post-MI, she develops sudden-onset sharp chest pain radiating to the back, hypotension (BP 90/60 mmHg), and muffled heart sounds. Echocardiography shows a large pericardial effusion with diastolic right atrial collapse. What is the most appropriate immediate next step?
A. Start high-dose corticosteroids and NSAIDs to reduce pericardial inflammation
B. Initiate intravenous fluid bolus and observe for spontaneous reabsorption of the effusion
C. Perform emergency pericardiocentesis followed by urgent cardiac surgery for free wall rupture repair
D. Obtain cardiac MRI to confirm the diagnosis and plan intervention
Explanation
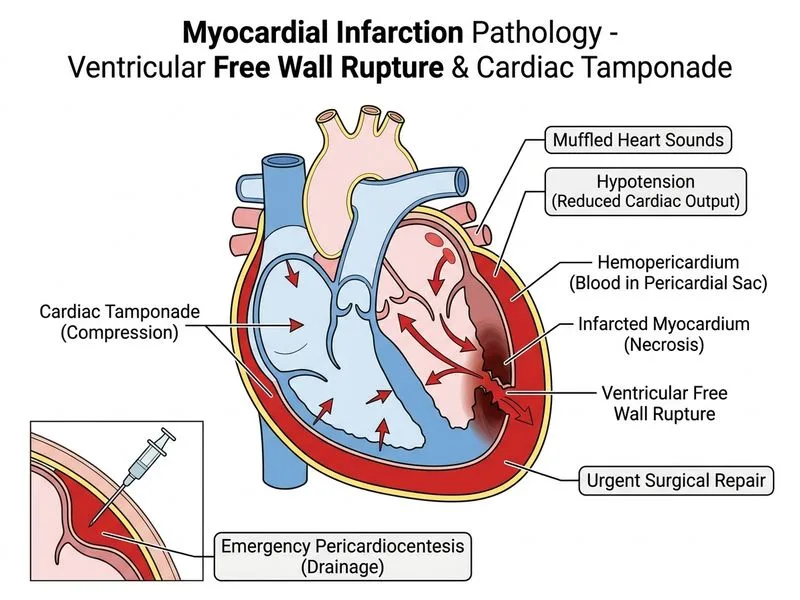
Clinical Diagnosis: Cardiac Tamponade from Free Wall Rupture
This patient has acute free wall rupture—a catastrophic mechanical complication of acute MI presenting with:
Sudden chest pain radiating to the back (rupture pain)
Hypotension and shock
Muffled heart sounds (Beck's triad)
Large pericardial effusion with diastolic RA collapse (echocardiographic signs of tamponade)
Pathophysiology
Key Point
Free wall rupture occurs when transmural myocardial necrosis extends through the full thickness of the ventricular wall, allowing blood to escape into the pericardial sac. This is a surgical emergency with mortality approaching 100% if untreated.
High-YieldNEET PG
Free wall rupture typically occurs 3–7 days post-MI (this case: day 3), when necrotic tissue is weakest. Risk factors include:
Anterior wall infarction (as in this case)
First MI (no collateral circulation)
Older age, female sex, hypertension
Successful reperfusion (paradoxically increases risk by allowing entry of inflammatory cells)
Management Algorithm
Loading diagram...
Immediate Management Steps
1. Pericardiocentesis (Temporizing)
Clinical Pearl
Pericardiocentesis is a life-saving temporizing measure, not definitive treatment. It relieves tamponade, restores cardiac output, and buys time for surgical preparation.
Perform at bedside under echocardiographic guidance
Drain fluid carefully (avoid rapid decompression, which can cause re-expansion pulmonary oedema)
Fluid is typically blood-stained or frank blood
2. Urgent Cardiac Surgery (Definitive)
Warning
Do NOT delay surgery for additional imaging (MRI, CT). This is a surgical emergency.
Surgical approach: median sternotomy
Repair: suture or patch the rupture site
May require cardiopulmonary bypass
Mortality even with immediate surgery is 30–50%; without surgery it is nearly 100%
Why Immediate Surgery Is Essential
Table
Intervention
Outcome
Pericardiocentesis alone
Temporary relief; patient will re-accumulate fluid and re-arrest
Medical management (fluids, inotropes)
Worsens tamponade; does not address rupture
Delayed surgery
Cardiogenic shock, cardiac arrest, death
Immediate surgery
Only chance of survival
Mnemonic: FREE WALL — Free wall rupture requires Rescue Emergency Echocardiography, then Wall repair And Life-saving Labor (surgery).
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.