The distinction between acute (0–12 h) and recent (12–48 h) MI depends on the dominant morphological features at each stage.
| Time Window | Dominant Feature | Microscopy |
|---|---|---|
| 0–4 hours | No light microscopic changes | Electron microscopy: mitochondrial swelling, glycogen loss |
| 4–12 hours | Coagulation necrosis + early neutrophils | Wavy fibers at border, hypereosinophilia |
| 12–48 hours | Contraction band necrosis + dense neutrophilic infiltrate | Hypercontracted sarcomeres, loss of striations |
| 2–7 days | Macrophage infiltration begins | Phagocytosis of dead myocytes |
| 1–2 weeks | Granulation tissue at margins | Fibroblasts, capillaries |
| >2 weeks | Fibrosis and collagen deposition | Scar formation |
Contraction band necrosis is the pathognomonic finding of the 12–48 hour window. It results from hypercontraction of viable myofibrils bordering dead tissue, creating dense eosinophilic bands with loss of normal striations. This distinguishes recent MI from acute MI, where coagulation necrosis dominates but contraction bands are absent or minimal.
Contraction band necrosis is also seen in reperfusion injury and catecholamine excess (e.g., pheochromocytoma crisis), not just MI. However, in the context of MI timing, it is the hallmark of the 12–48 hour phase.
For NEET PG, memorize the 4-hour rule: no light microscopic changes in the first 4 hours. Contraction bands appear by 12 hours and peak at 24–48 hours.
Loading illustration…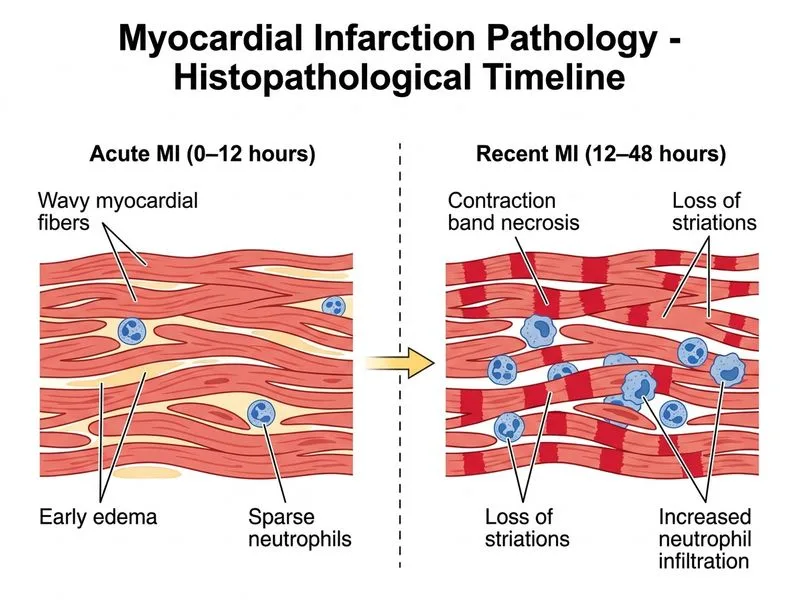
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →