The depth and extent of myocardial necrosis fundamentally distinguish these two patterns and correlate with the clinical presentation and prognosis.
| Feature | Transmural MI | Subendocardial MI |
|---|---|---|
| Depth of necrosis | Full thickness (endocardium to epicardium) | Inner third of myocardium only |
| Typical cause | Complete coronary occlusion | Severe stenosis, demand ischemia, or reperfusion |
| ECG finding | ST elevation + pathological Q waves | ST depression, T-wave inversion (no Q waves) |
| Complication risk | High (rupture, aneurysm, VSD) | Lower |
| Epicardial involvement | Yes (defines transmural) | No |
| Pericarditis risk | High (transmural necrosis irritates pericardium) | Low |
Full-thickness involvement including the epicardium is the defining pathological criterion for transmural MI. In this case, complete RCA occlusion (inferior STEMI) typically causes transmural necrosis in the inferior wall.
Transmural MI carries higher risk of mechanical complications (free wall rupture, ventricular septal defect, papillary muscle rupture) because the necrosis extends through all layers, weakening the structural integrity of the wall.
Remember the depth rule: Transmural = full thickness (endocardium + epicardium); Subendocardial = inner third only. This distinction is testable in both pathology and clinical reasoning questions.
TRANSMURAL = THROUGH-ALL — necrosis extends through all layers of the myocardium.
Loading illustration…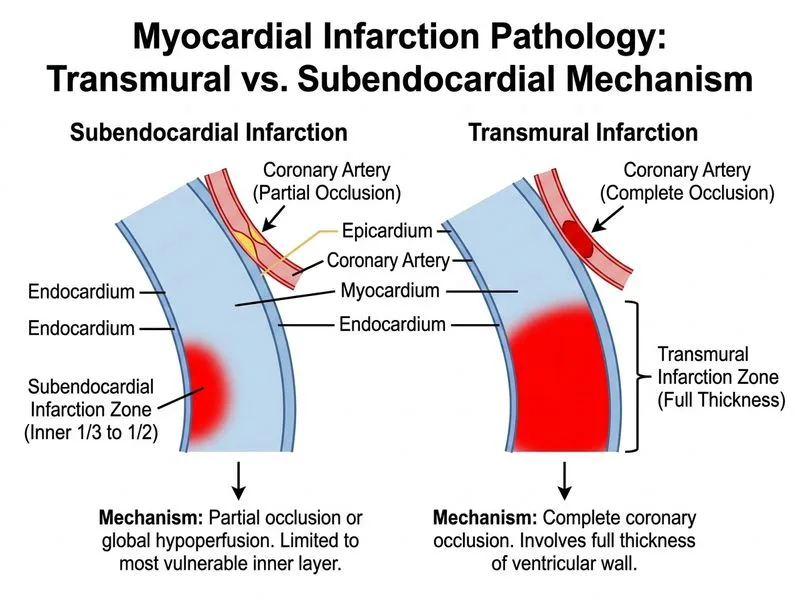
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →