Neonatal Jaundice MCQ — NEET PG Practice Question | NEETPGAI
Neonatal Jaundice
medium
smile Pediatrics
A 5-day-old female neonate, born to an O-positive, antibody screen-negative mother, presents with jaundice. The infant is exclusively breastfed with good latch and feeds 10–12 times daily. Weight is 3.4 kg (birth weight 3.5 kg). Stool output is 4–5 stools per day, and urine output is normal. Direct antiglobulin test (DAT) is negative. Total serum bilirubin is 16 mg/dL, conjugated bilirubin 0.3 mg/dL. What is the most appropriate next step in management?
A. Discontinue breastfeeding and switch to formula
B. Obtain a reticulocyte count and peripheral blood smear
C. Perform exchange transfusion immediately
D. Continue breastfeeding and initiate phototherapy; reassess bilirubin in 24 hours
Explanation
Clinical Analysis
Key Clinical Features
Age: Day 5 (late-onset jaundice)
Feeding: Exclusive breastfeeding with good latch, 10–12 times/day — adequate intake
Weight loss: Minimal (2.9%) — within normal range
Stool output: 4–5 stools/day — normal
DAT: Negative — rules out hemolytic disease
Bilirubin: 16 mg/dL at day 5 — above phototherapy threshold for this age/weight
Diagnosis: Breast Milk Jaundice
Key Point
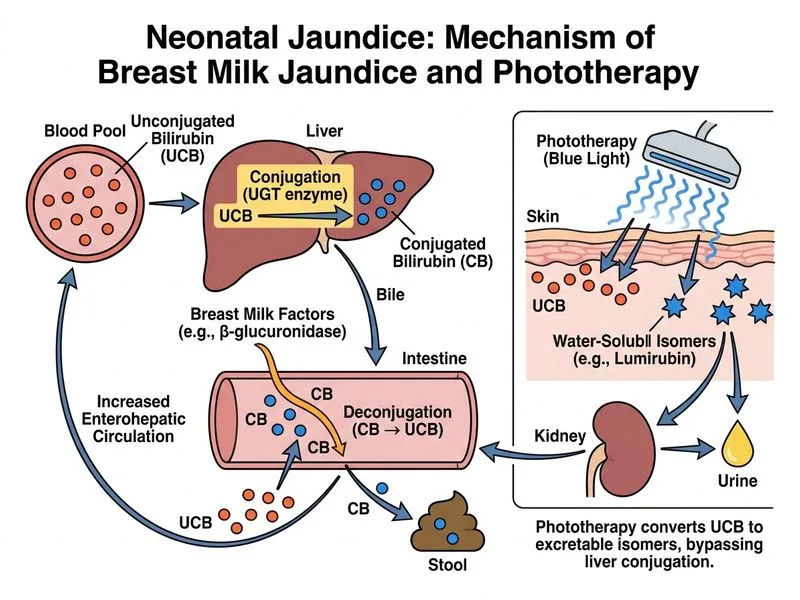
Breast milk jaundice (also called "late-onset breastfeeding jaundice") occurs in infants with adequate milk intake but elevated bilirubin due to substances in breast milk (β-glucuronidase, lipase) that increase enterohepatic circulation of bilirubin. It presents on day 4–7+ with normal weight, normal stool output, and negative DAT.
Phototherapy Threshold for Day 5
For a healthy term infant (≥35 weeks) at day 5:
Phototherapy threshold ≈ 15 mg/dL (varies slightly by weight and risk category)
This infant's bilirubin of 16 mg/dL exceeds the threshold and requires phototherapy
Clinical Pearl
Breast milk jaundice is NOT a contraindication to breastfeeding. In fact, continuing breastfeeding while providing phototherapy is the standard of care. The goal is to increase milk intake (which increases stool output and bilirubin excretion) while simultaneously reducing bilirubin production with phototherapy.
Why NOT Discontinue Breastfeeding?
1.
Adequate intake is already established — latch is good, frequency is 10–12 times/day
2.
Breast milk has immunological and nutritional benefits — switching to formula removes these
3.
Increased breastfeeding frequency (not cessation) helps resolve breast milk jaundice
4.
Lactation support is more effective than formula supplementation
High-YieldNEET PG
The distinction between breastfeeding jaundice (poor intake → discontinue, fix latch) and breast milk jaundice (adequate intake → continue, add phototherapy) is critical for exam success.