Neonatal Jaundice MCQ — NEET PG Practice Question | NEETPGAI
Neonatal Jaundice
hard
smile Pediatrics
A 5-day-old preterm neonate (32 weeks gestation) presents with progressive jaundice. Serum total bilirubin is 12 mg/dL with a conjugated fraction of 1.2 mg/dL (10%). Direct antiglobulin test is negative. Feeding history is poor with weight loss of 12%. Which investigation is most appropriate to identify the underlying cause?
A. Thyroid-stimulating hormone (TSH) and free T4
B. Reticulocyte count and peripheral blood smear
C. Urine reducing substances and urine culture
D. Liver function tests and abdominal ultrasound
Explanation
Investigation of Choice for Unconjugated Hyperbilirubinemia in Preterm Neonate
Why Reticulocyte Count and Peripheral Blood Smear are Correct
High-YieldNEET PG
In a preterm neonate with unconjugated hyperbilirubinemia and a negative DAT, the most important next step is to evaluate for non-immune hemolytic causes, which are the most common and clinically significant causes of pathologic jaundice in preterm neonates:
1.
G6PD deficiency — the most common enzyme deficiency causing neonatal jaundice; DAT is negative; reticulocyte count is elevated; peripheral smear shows bite cells/blister cells
ABO incompatibility — can have a weakly positive or negative DAT; smear shows microspherocytes; elevated reticulocytes
4.
Pyruvate kinase deficiency — DAT negative; elevated reticulocytes
Clinical Pearl
A negative DAT rules out immune-mediated hemolysis (Rh, Kell, Duffy incompatibility) but does NOT rule out non-immune hemolysis. In a preterm neonate with progressive unconjugated hyperbilirubinemia, reticulocyte count and peripheral smear are the first-line investigations to identify the underlying cause (Nelson Textbook of Pediatrics, 21e, Ch 102).
Why Other Options Are Less Appropriate
Table
Investigation
Yield in This Case
Rationale
Reticulocyte count + peripheral smear
High
Identifies non-immune hemolysis (G6PD, spherocytosis, ABO) — most common cause of pathologic unconjugated hyperbilirubinemia with negative DAT
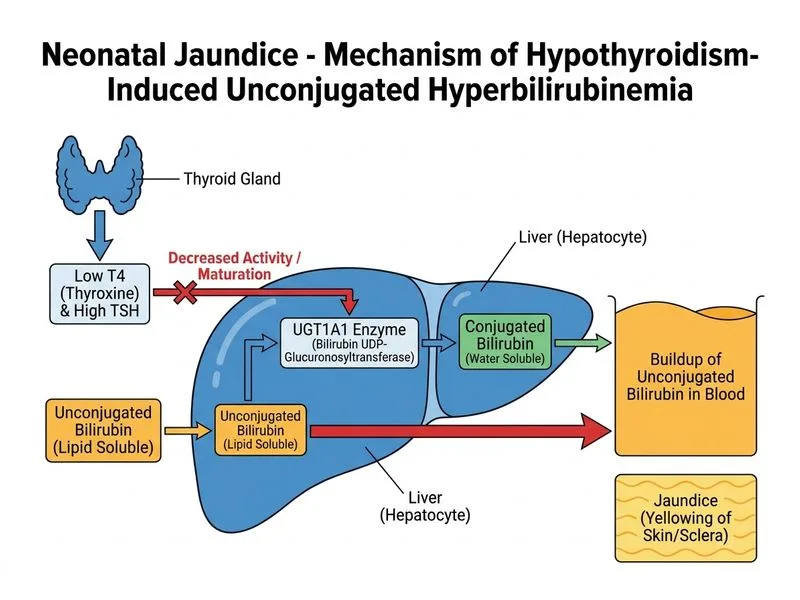
TSH + Free T4
Lower priority
Hypothyroidism is a cause of prolonged jaundice but is part of universal newborn screening; it does not explain acute progressive jaundice in a 5-day-old as the primary investigation
Urine reducing substances + urine culture
Low
Galactosemia causes conjugated hyperbilirubinemia; UTI is possible but less likely as the primary cause here
LFTs + abdominal USG
Low
Appropriate for conjugated hyperbilirubinemia (>20% direct fraction); conjugated fraction here is only 10%
Diagnostic Approach Algorithm
Step 1: Confirm unconjugated hyperbilirubinemia ✓ (conjugated = 10%) Step 2: DAT negative → exclude immune hemolysis ✓ Step 3: → Reticulocyte count + peripheral smear to identify non-immune hemolysis Step 4: If reticulocyte count elevated → G6PD assay, osmotic fragility test Step 5: If reticulocyte count normal → consider poor intake, prematurity, hypothyroidism (TSH/T4)
Key Point
The investigation that is "most appropriate to identify the underlying cause" in a DAT-negative preterm neonate with progressive unconjugated hyperbilirubinemia is reticulocyte count and peripheral blood smear, as non-immune hemolysis is the most common identifiable pathologic cause.
Nelson Textbook of Pediatrics 21e Ch 102; Cloherty's Manual of Neonatal Care 8e Ch 26
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.