## Clinical Scenario Analysis This patient presents with **painless progressive jaundice** with a **dilated CBD (12 mm) and normal gallbladder** — classic for **distal bile duct obstruction** (likely pancreatic head malignancy or distal CBD stricture). The absence of stones and fever rules out acute cholecystitis. ## Diagnostic Approach to Obstructive Jaundice **Key Point:** The imaging hierarchy in obstructive jaundice depends on the clinical suspicion and ultrasound findings. | Investigation | Indication | Sensitivity | Role | |---|---|---|---| | **MRCP** | Suspected CBD obstruction; need ductal anatomy without intervention | 85–95% | Gold standard for diagnosis; non-invasive; defines anatomy | | **ERCP** | Confirmed CBD obstruction; therapeutic intent (stone extraction, stent placement) | 90–95% | Therapeutic modality; not diagnostic-only | | **CT** | Suspected malignancy; assess resectability; local staging | 70–80% | Staging tool; less sensitive for small stones | | **Hepatobiliary scintigraphy** | Suspected biliary dyskinesia; assess cystic duct patency | Low | Not for obstruction diagnosis | ## Why MRCP Is Correct **High-Yield:** MRCP is the **non-invasive gold standard** for defining the **site, nature, and extent** of bile duct obstruction. In this case: 1. **Ultrasound has already confirmed obstruction** (dilated CBD, normal gallbladder). 2. **MRCP will identify the cause** — pancreatic mass, distal stricture, or other lesion — **without risk of pancreatitis** (which ERCP carries in 3–7% of cases). 3. **MRCP provides ductal anatomy** needed for surgical planning (if malignancy) or further intervention. 4. **ERCP should be reserved for therapeutic intervention** (e.g., stone extraction, stent placement), not diagnostic confirmation alone. **Clinical Pearl:** In painless jaundice with dilated CBD and normal gallbladder, always suspect **pancreatic head malignancy** until proven otherwise. MRCP will show the distal obstruction pattern and allow assessment of the pancreatic parenchyma. ## Why Other Options Are Suboptimal - **CT:** Useful for staging suspected malignancy *after* diagnosis is confirmed by MRCP; not the first-line diagnostic tool for defining ductal anatomy. - **ERCP:** Carries pancreatitis risk and is therapeutic, not diagnostic-only; reserved for when intervention (stone removal, stent) is planned. - **Hepatobiliary scintigraphy:** Assesses cystic duct patency and biliary dyskinesia; not useful for obstruction diagnosis. 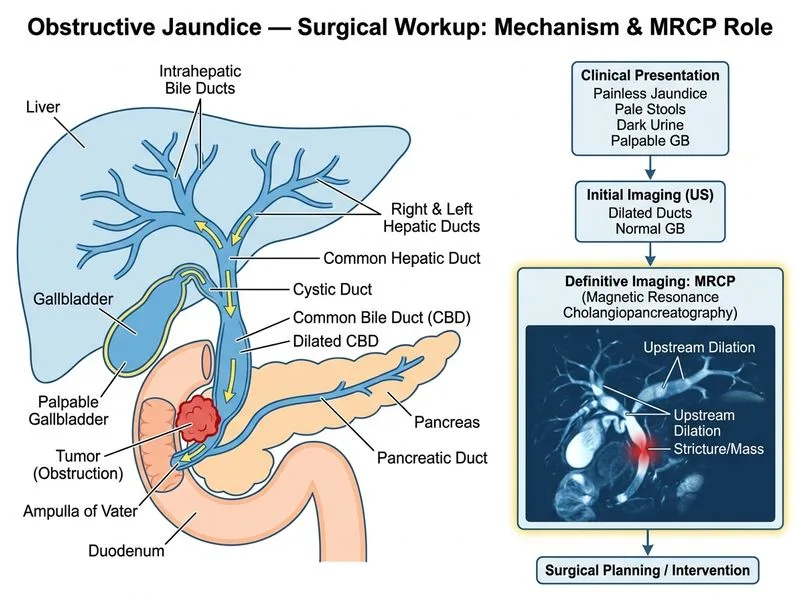
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.