## Clinical Scenario Analysis This patient presents with **painless progressive jaundice, weight loss, and the "double duct sign"** (dilated CBD + dilated pancreatic duct) — **pathognomonic for pancreatic head malignancy**. MRCP has already confirmed the diagnosis morphologically. The next critical step is **staging to determine resectability** before committing to surgery. ## Surgical Workup Algorithm for Pancreatic Head Obstruction ```mermaid flowchart TD A["Painless jaundice + double duct sign"]:::outcome --> B["MRCP/EUS confirms mass"]:::outcome B --> C{"Resectability assessment needed?"}:::decision C -->|"Yes: CT staging first"| D["CT chest/abdomen/pelvis with IV contrast"]:::action D --> E{"Locally advanced or metastatic?"}:::decision E -->|"No: Resectable"| F["Proceed to pancreaticoduodenectomy"]:::action E -->|"Yes: Unresectable"| G["Palliative biliary stent + chemotherapy"]:::action C -->|"Already staged"| H["Surgical planning"]:::action ``` ## Why CT Staging Is the Correct Next Step **High-Yield:** Before any major resection, **CT with IV contrast is mandatory** to: 1. **Assess vascular involvement** — encasement of superior mesenteric vessels, portal vein, or hepatic artery (contraindication to curative resection). 2. **Detect distant metastases** — liver, peritoneum, or distant lymph nodes (upstages to unresectable). 3. **Evaluate local extent** — involvement of duodenum, stomach, colon (affects surgical approach). 4. **Guide operative planning** — vessel reconstruction, extent of resection. **Key Point:** Approximately **80–90% of pancreatic cancers are unresectable at presentation** due to vascular invasion or metastatic disease. CT identifies these patients *before* unnecessary surgery. **Clinical Pearl:** The "double duct sign" on MRCP is highly specific for pancreatic head cancer but does NOT guarantee resectability. Staging CT is non-negotiable before pancreaticoduodenectomy. ## Why Other Options Are Premature or Incorrect | Option | Why It's Wrong | |---|---| | **Proceed directly to surgery** | Violates the principle of staging before major resection. 80% of patients are unresectable; CT would have prevented unnecessary laparotomy. | | **EUS with FNA** | Tissue diagnosis is already established by imaging (MRCP + clinical context). FNA adds time and cost without changing management. Staging takes priority. | | **PTC with stent** | Palliative biliary drainage is reserved for *unresectable* disease or patients unfit for surgery. Premature stenting before staging may complicate future resection and delays definitive assessment. | **Mnemonic for Pancreatic Cancer Workup:** **"STAGE before SCALPEL"** - **S**taging CT (chest/abdomen/pelvis) - **T**issue diagnosis (if needed; often imaging suffices) - **A**ssess resectability (vascular, metastatic) - **G**uide operative plan - **E**xecute surgery (only if resectable) ## Resectability Criteria (CT-Based) **Resectable:** No vascular involvement, no distant metastases, no major organ invasion. **Borderline resectable:** Venous involvement (SMV/PV) without occlusion; short segment of arterial contact (HA/SMA) without encasement. **Unresectable:** Vascular encasement/occlusion, distant metastases, peritoneal carcinomatosis, major organ invasion. 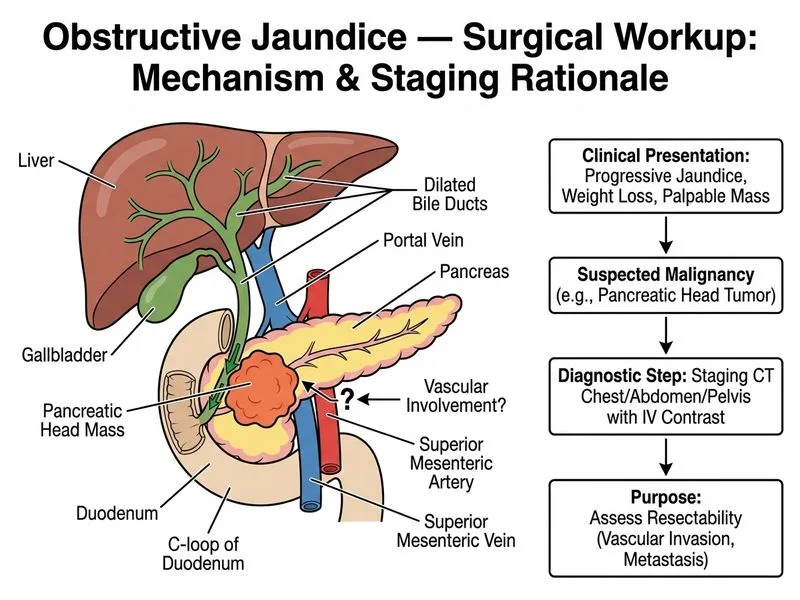
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.