## Clinical Scenario Analysis This patient presents with **obstructive jaundice** characterized by: - Painless, progressive jaundice (3 weeks) - Pale stools and dark urine (conjugated hyperbilirubinemia) - Markedly elevated ALP and GGT (cholestasis pattern) - Dilated bile ducts on ultrasound - **No stone visualized on ultrasound** - **Normal pancreatic head on ultrasound** ## Diagnostic Approach to Obstructive Jaundice **Key Point:** The absence of a visible stone on ultrasound in a patient with dilated ducts and obstructive jaundice raises suspicion for **malignant obstruction** (pancreatic cancer, cholangiocarcinoma, ampullary cancer) rather than choledocholithiasis. **High-Yield:** The **Courvoisier sign** (palpable gallbladder in painless jaundice) suggests malignancy rather than stone disease, because in chronic stone disease, the gallbladder is typically fibrosed and non-distensible. This patient has dilated ducts without a visible stone — a red flag for malignancy. ## Why CT Abdomen with Contrast is the Next Step 1. **Sensitivity for pancreatic and biliary malignancy:** CT with contrast is the first-line cross-sectional imaging to detect pancreatic head masses, cholangiocarcinoma, and assess for metastases. 2. **Characterizes the obstruction:** Defines whether the obstruction is at the level of the CBD, ampulla, or pancreatic head. 3. **Staging:** Provides information about local invasion and distant spread if malignancy is present. 4. **Guides further intervention:** Results determine whether ERCP, PTC, or surgical exploration is most appropriate. ## Investigation Algorithm for Obstructive Jaundice ```mermaid flowchart TD A[Obstructive Jaundice + Dilated Ducts]:::outcome --> B{Stone visible on ultrasound?}:::decision B -->|Yes| C[ERCP with sphincterotomy]:::action B -->|No| D[CT abdomen with contrast]:::action D --> E{Malignancy suspected?}:::decision E -->|Yes| F[Staging + Surgical/Palliative planning]:::action E -->|No| G[Consider PTC or ERCP for tissue diagnosis]:::action E -->|Inconclusive| H[ERCP ± tissue sampling]:::action ``` **Clinical Pearl:** In painless obstructive jaundice without a visible stone, **always rule out malignancy first** before pursuing ERCP. ERCP carries a 3–5% risk of pancreatitis and should not be done without a clear indication. **Tip:** Remember the **"painless jaundice triad"** → suspect malignancy: - Painless progressive jaundice - Dilated ducts - No stone on imaging ## Why Not ERCP Immediately? ERCP is **therapeutic** for choledocholithiasis but is **diagnostic** for malignancy only if tissue is obtained (brush cytology, biopsy). In this case, CT should precede ERCP to: - Rule out unresectable malignancy (avoiding unnecessary ERCP) - Identify the exact level and nature of obstruction - Plan the appropriate intervention (ERCP, PTC, or surgery) [cite:Sabiston Textbook of Surgery 21e Ch 54] 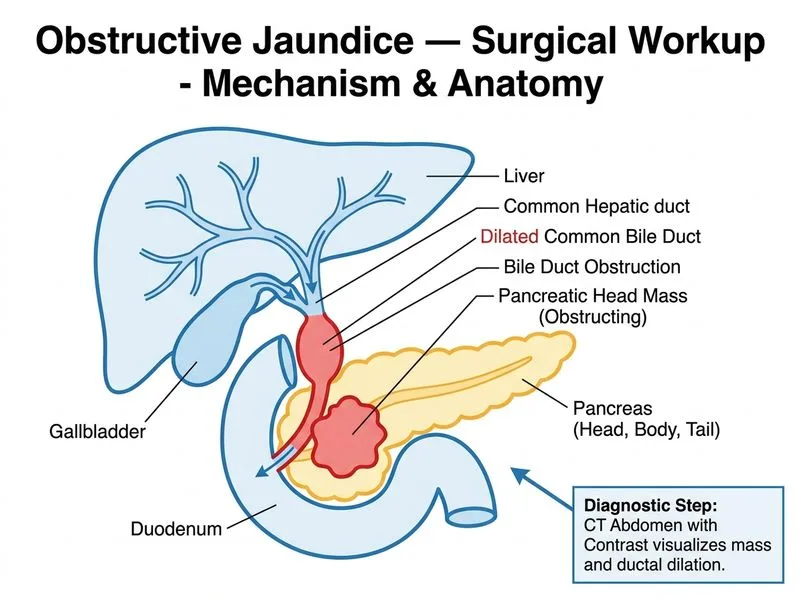
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.