## Clinical Diagnosis This patient has **acute cholangitis** (Charcot's triad: fever, jaundice, RUQ pain) secondary to **CBD stone obstruction in a PSC patient**. The diagnosis is confirmed by: - Fever + jaundice + RUQ pain (Charcot's triad) - Elevated transaminases and ALP (cholestasis) - Leukocytosis - Imaging evidence of stone + dilated ducts ## Acute Cholangitis: Urgent Intervention Required ```mermaid flowchart TD A[Acute cholangitis: fever + jaundice + obstruction]:::urgent --> B{Hemodynamically stable?}:::decision B -->|Yes| C[ERCP within 24 hours]:::action B -->|No| D[Resuscitation + antibiotics]:::action D --> E[ERCP within 12 hours]:::action C --> F[Sphincterotomy + stone extraction]:::action E --> F F --> G[Biliary drainage achieved]:::outcome ``` ## Why ERCP Is the Gold Standard **High-Yield:** ERCP with endoscopic sphincterotomy and stone extraction is the **first-line definitive treatment** for acute cholangitis due to CBD obstruction. Success rate >90%, morbidity <5% in experienced hands. **Key Point:** Acute cholangitis is a **surgical emergency**. Delay in biliary drainage increases mortality from sepsis. ERCP should be performed **within 24 hours** (ideally <12 hours in unstable patients). **Mnemonic: ERCP in Acute Cholangitis — STAT:** - **S**tone extraction or other obstruction relief - **T**herapeutic (not diagnostic) - **A**cute presentation (fever + obstruction) - **T**ime-critical (within 24 hours) ## Comparison of Drainage Modalities | Modality | Indication | Timing | Success | Morbidity | |----------|-----------|--------|---------|----------| | **ERCP + sphincterotomy** | Distal CBD obstruction, stable patient | <24 hrs | >90% | <5% | | **PTC + drainage** | ERCP failure, hilar obstruction, intrahepatic stones | <24 hrs | 85–90% | 5–10% | | **Open choledochotomy** | ERCP failure, perforation, anatomic contraindication | <24 hrs | 95% | 10–15% | | **Supportive care alone** | Mild cholangitis without sepsis (rare) | — | Mortality 5–10% | High | ## Why Other Options Are Incorrect **Option 2 (PTC):** Reserved for ERCP failure, hilar strictures, or intrahepatic stones. Not first-line in distal CBD obstruction. **Option 3 (Open surgery):** Invasive, higher morbidity. Reserved for ERCP failure or perforation. **Option 4 (Delayed ERCP):** **Dangerous.** Acute cholangitis with sepsis requires urgent drainage. Delaying 48–72 hours risks fulminant sepsis, organ failure, and death. **Clinical Pearl:** In PSC patients, recurrent cholangitis is common due to multiple strictures and stones. ERCP may need to be repeated; consider long-term ursodeoxycholic acid and surveillance. [cite:Harrison 21e Ch 310; Schwartz's Principles of Surgery 11e Ch 33] 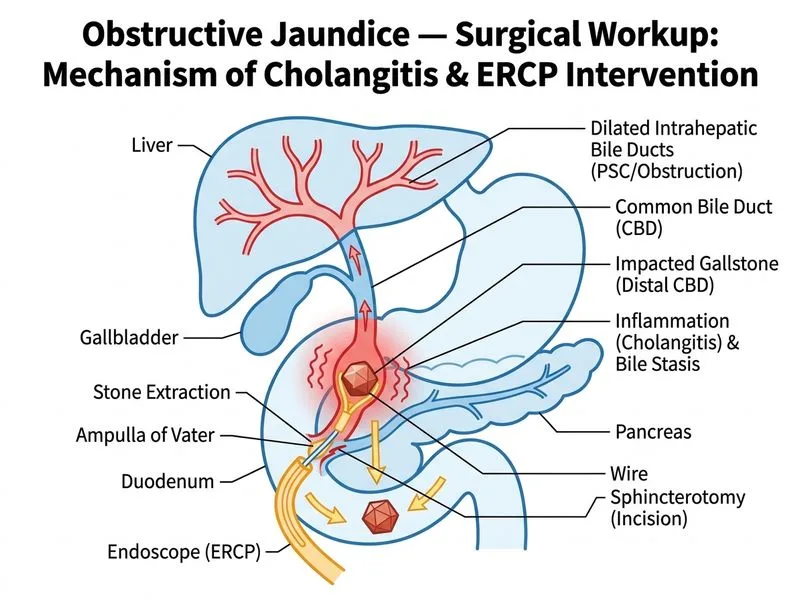
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.