A 28-year-old male construction worker sustains a crush injury to his right tibia from a falling steel beam at a construction site in Delhi. On arrival at the emergency department, there is a 4 cm laceration over the anterior tibia with bone protruding through the skin. The wound is heavily contaminated with soil and debris. Neurovascular examination reveals intact dorsalis pedis pulse and normal motor/sensory function. What is the most appropriate immediate next step in management?
A. Skeletal traction application followed by delayed surgical intervention after soft tissue healing
B. Immediate open reduction and internal fixation with plate and screws
C. Application of a sterile dressing and transfer to the operating theatre for definitive fixation
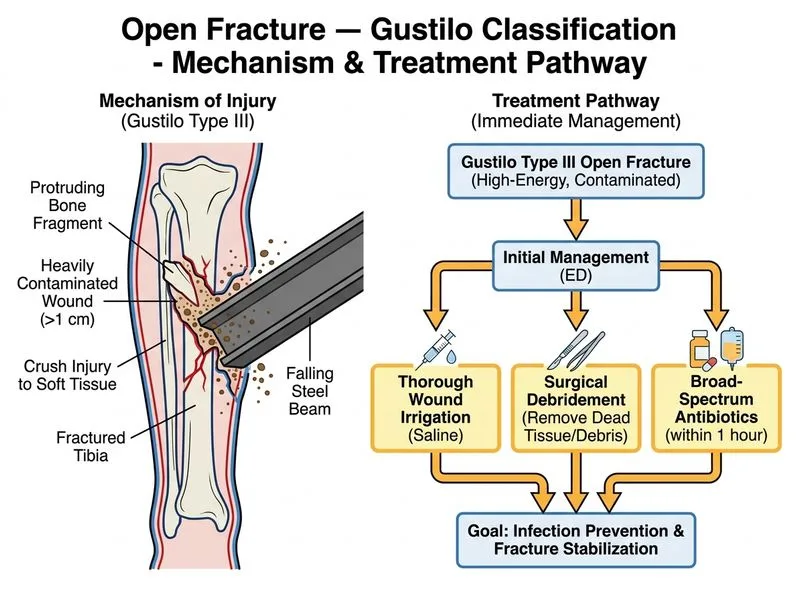
D. Thorough wound irrigation, debridement, and administration of broad-spectrum antibiotics within 1 hour
Explanation
Immediate Management of Open Fractures
Key Point
The golden period for open fracture management is the first 6–8 hours, with antibiotics ideally given within 1 hour of injury. Gustilo Type III (or even Type II) fractures require urgent irrigation, debridement, and antibiotic coverage before any definitive fixation.
Gustilo Classification Hierarchy
Table
Type
Wound Size
Contamination
Soft Tissue Damage
Fracture Pattern
I
< 1 cm
Minimal
Minimal
Simple
II
1–10 cm
Moderate
Moderate
Simple or comminuted
III
> 10 cm OR high-energy
Heavy (soil/debris)
Extensive
Comminuted; vascular injury possible
This patient has a Type II or Type III open fracture (4 cm laceration, bone exposure, heavy soil contamination).
Immediate Action Sequence
1.
Antibiotics first — broad-spectrum IV (e.g., cephalosporin + aminoglycoside ± clindamycin for soil organisms) within 1 hour
2.
Wound irrigation and debridement — remove devitalized tissue, foreign material, and contamination in the operating theatre
3.
Stabilization — temporary external fixation or splinting; definitive fixation deferred until soft tissue is viable
4.
Tetanus prophylaxis — always
High-YieldNEET PG
The sequence is NOT immediate fixation. Contaminated open fractures must be cleaned first to prevent osteomyelitis and gas gangrene.
Clinical Pearl
Soil contamination carries risk of Clostridium species (gas gangrene) — clindamycin or penicillin is mandatory in addition to broad-spectrum cover.
Why Immediate ORIF Is Wrong
Premature fixation in a contaminated wound risks:
Implant-related infection
Osteomyelitis
Sepsis
Loss of limb
Debridement and soft tissue assessment must precede implant placement.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.