The Gustilo and Anderson classification system stratifies open fractures by wound size, soft tissue damage, contamination, and vascular injury — each factor predicts infection risk and functional outcome.
| Feature | Type I | Type II | Type III |
|---|---|---|---|
| Wound size | <1 cm | 1–10 cm | >10 cm OR extensive |
| Soft tissue damage | Minimal | Moderate | Severe, devascularized |
| Contamination | Minimal | Moderate | High (farm, marine, etc.) |
| Vascular injury | Absent | Absent | May be present |
| Infection risk | 0–6% | 2–16% | 25–50% |
Type I is essentially a "clean" open fracture — the bone has broken through the skin, but the wound tract is small and the surrounding soft tissues are largely intact. Type II involves more extensive soft tissue trauma, a larger wound, and greater contamination risk — but still lacks the severe devascularization or vascular injury seen in Type III.
Rockwood & Green's Fractures in Adults 9e Ch 12
Loading illustration…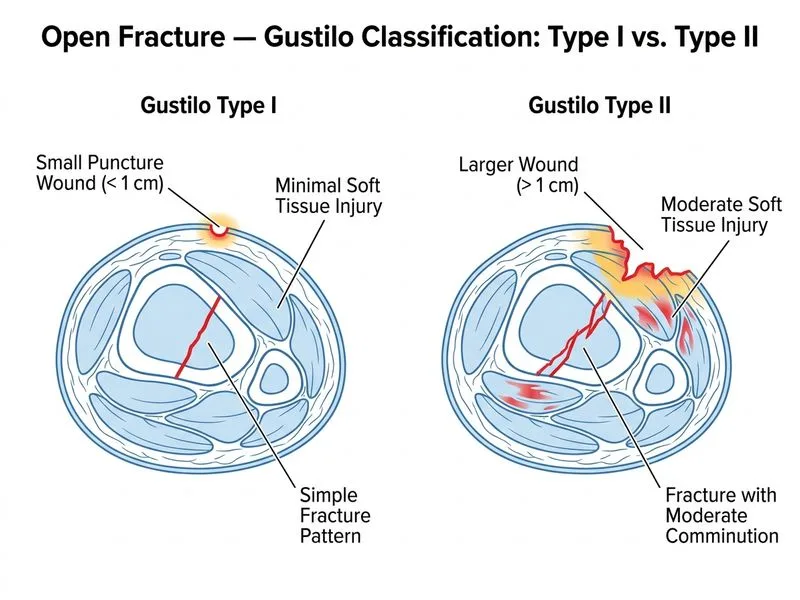
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →