Orbital Cellulitis MCQ — NEET PG Practice Question | NEETPGAI
Orbital Cellulitis
easy
eye Ophthalmology
Which of the following is the most common predisposing factor for orbital cellulitis in children?
A. Ethmoid sinusitis
B. Maxillary sinusitis
C. Sphenoid sinusitis
D. Frontal sinusitis
Explanation
Predisposing Factors in Orbital Cellulitis
Key Point
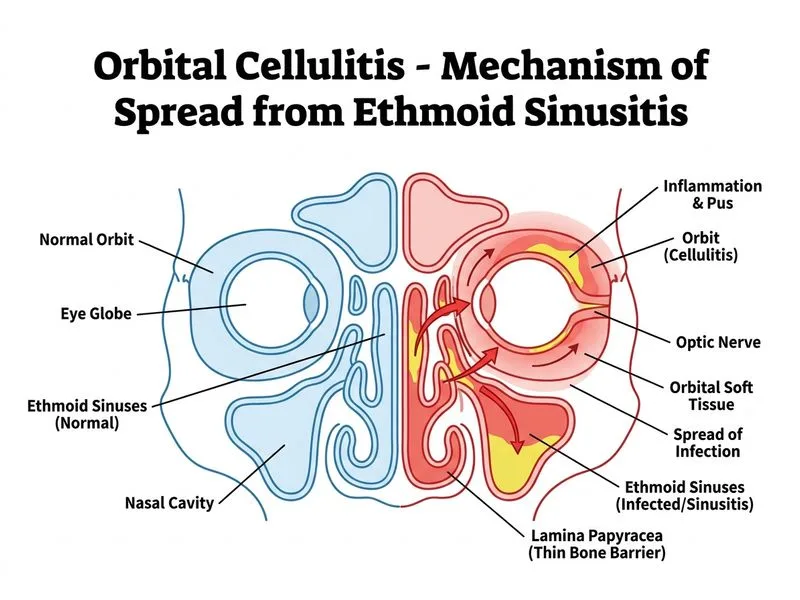
Ethmoid sinusitis is the most common source of orbital cellulitis in children, accounting for approximately 50–70% of cases.
Anatomical Basis
The ethmoid sinus has several features that make it a frequent source of orbital spread:
1.
Thin lamina papyracea — The medial orbital wall is composed of a thin bone (lamina papyracea) that separates the ethmoid air cells from the orbit, allowing rapid bacterial spread.
Proximity to orbit — The ethmoid sinus is directly adjacent to the medial orbit, unlike maxillary or frontal sinuses.
Frequency by Sinus
Table
Sinus
Frequency
Reason
Ethmoid
50–70%
Thin lamina papyracea, direct adjacency
Maxillary
10–20%
Thicker bone, less direct communication
Sphenoid
5–10%
Posterior location, rarer involvement
Frontal
5–10%
Superior location, less common source
Clinical Pearl
In children, acute ethmoid sinusitis progressing to orbital cellulitis is a medical emergency requiring urgent imaging (CT orbit) and broad-spectrum antibiotics to prevent vision-threatening complications.
High-YieldNEET PG
Remember the "thin lamina papyracea" as the anatomical key — it is the weakest barrier between the ethmoid sinus and the orbit.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.