Orbital Cellulitis MCQ — NEET PG Practice Question | NEETPGAI
Orbital Cellulitis
hard
eye Ophthalmology
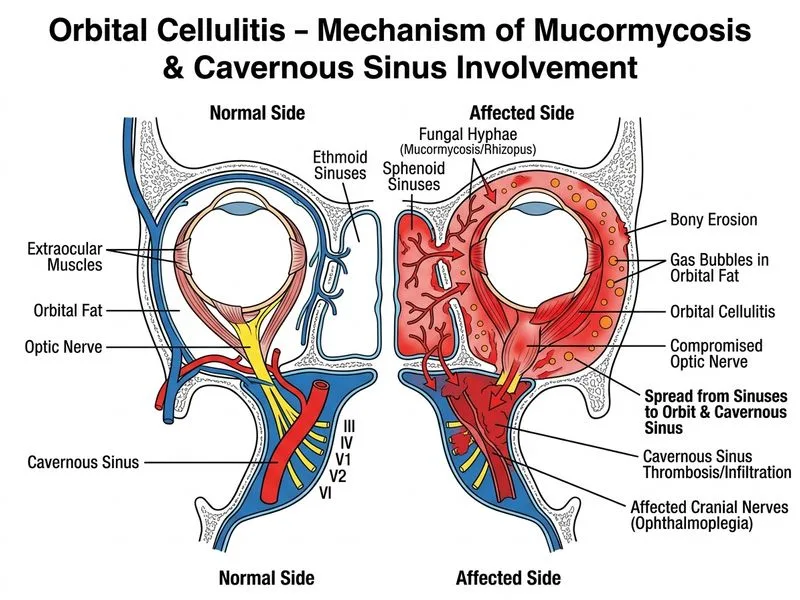
A 45-year-old man with poorly controlled diabetes and chronic sinusitis presents with acute right eye pain, proptosis, and chemosis. On examination, he has restricted eye movements and a mid-dilated pupil that does not react to light. Fundoscopy shows retinal whitening and optic disc swelling. CT orbit shows infiltration of the right cavernous sinus with gas bubbles in the orbital fat. Blood glucose is 480 mg/dL. What is the most likely diagnosis, and which organism is classically associated?
A. Mucormycosis with cavernous sinus involvement; *Rhizopus* species
B. Acute orbital abscess with gas-forming organism; *Escherichia coli*
C. Acute ethmoid cellulitis with secondary cavernous sinus thrombosis; *Staphylococcus aureus*
Preseptal cellulitis with orbital extension; *Streptococcus pyogenes*
D.
Explanation
Clinical Diagnosis: Rhinocerebral Mucormycosis
Key Clinical Features
High-YieldNEET PG
The triad of uncontrolled diabetes + gas in orbit + rapid cavernous sinus involvement is pathognomonic for mucormycosis.
Risk Factors & Epidemiology
Table
Risk Factor
Mechanism
Relevance
Uncontrolled diabetes (DKA/HHS)
Impaired neutrophil function, elevated glucose
Most common risk factor
Hematologic malignancy
Immunosuppression
Second most common
Solid organ/stem cell transplant
T-cell depletion
High risk
Prolonged corticosteroid use
Immune dysregulation
Moderate risk
Clinical Pearl
This patient's blood glucose of 480 mg/dL with poor glycemic control is the critical predisposing factor. Mucormycosis is an opportunistic infection that thrives in hyperglycemic, acidotic states.
Pathognomonic Features of Orbital Mucormycosis
1.
Gas in orbital fat (angioinvasion → tissue necrosis → gas-forming organisms)
2.
Rapid progression to cavernous sinus thrombosis (within days)
3.
Ophthalmoplegia with mid-dilated pupil (CN III palsy from cavernous sinus involvement)
4.
Retinal whitening (cotton-wool spots from retinal ischemia due to vascular invasion)
5.
Black necrotic tissue in nasal mucosa or palate (pathognomonic but late sign)
Organism Identification
Mnemonic
RHIZOMUCOR — The three most common causative agents:
Rhizopus species (60–70% of cases)
Mucor species (20–30%)
Rhizomucor species (5–10%)
All are angioinvasive fungi that cause:
Vascular thrombosis → tissue necrosis
Rapid spread to sinuses, orbit, brain
Fulminant course without urgent intervention
Pathophysiology
Loading diagram...
Diagnostic Approach
Key Point
Diagnosis requires:
1.
High clinical suspicion (diabetes + rapid orbital cellulitis + gas on imaging)
2.
Tissue biopsy with histopathology (broad, non-septate hyphae with right-angle branching)
Start immediately (do NOT wait for culture confirmation)
Continue until clinical improvement, then switch to posaconazole
2.
Oral Posaconazole (maintenance after IV induction)
Dose: 300 mg daily in divided doses
Duration: Months to years depending on extent
3.
Aggressive Glycemic Control
Insulin therapy to achieve glucose <200 mg/dL
Correct metabolic acidosis if present
Critical for immune recovery
Surgical Management
Warning
Surgery is mandatory and often requires multiple debridements:
Endoscopic sinus debridement (remove all necrotic tissue)
Orbital debridement if abscess present
Repeat procedures every 48–72 hours until no new necrosis
Prognosis
Clinical Pearl
Even with aggressive treatment, mortality is 20–50% in diabetic patients with cavernous sinus involvement. Early recognition and immediate intervention are critical for vision and life preservation.
Kanski Clinical Ophthalmology 9e Ch 6; Harrison 21e Ch 199
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.