Orbital Cellulitis MCQ — NEET PG Practice Question | NEETPGAI
Orbital Cellulitis
medium
eye Ophthalmology
A 32-year-old man from Delhi presents with acute onset proptosis, chemosis, ophthalmoplegia, and fever for 2 days. He reports a history of rhinosinusitis 1 week ago. On examination, visual acuity is 6/9 in both eyes, intraocular pressure is elevated, and fundus shows early disc edema. Blood cultures are pending. What is the most appropriate immediate next step in management?
A. Start topical antibiotics and oral NSAIDs; observe for 48 hours
B. Arrange urgent surgical drainage of the orbit without imaging
C. Perform lumbar puncture to rule out meningitis before starting antibiotics
D. Start broad-spectrum intravenous antibiotics (ceftriaxone + vancomycin) and arrange urgent CT/MRI orbit
Explanation
Clinical Context
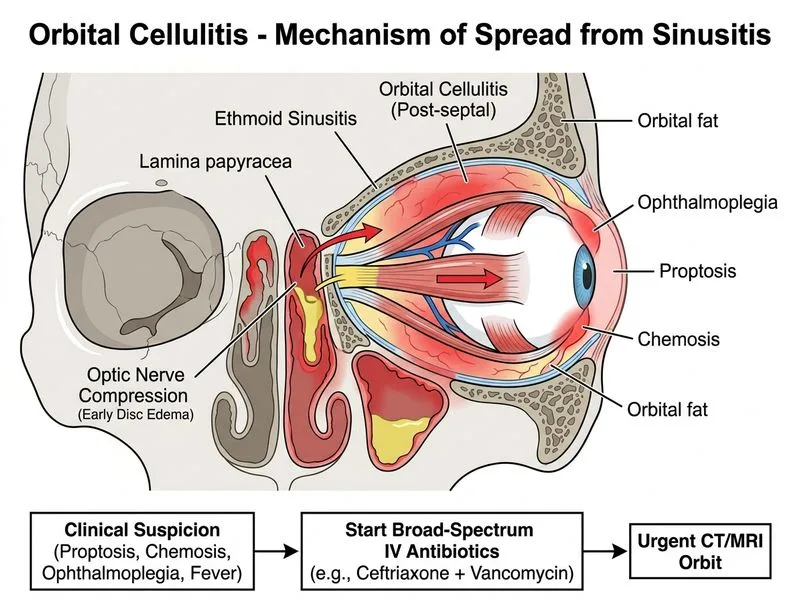
This patient presents with classic signs of acute orbital cellulitis: proptosis, chemosis, ophthalmoplegia, fever, and a clear predisposing factor (recent rhinosinusitis). The elevated intraocular pressure and early disc edema indicate orbital involvement with risk of vision loss.
Management Algorithm for Orbital Cellulitis
Loading diagram...
Key Management Principles
Key Point
Orbital cellulitis is a medical emergency. The standard of care is immediate empiric IV broad-spectrum antibiotics (ceftriaxone 2 g IV 6-hourly + vancomycin 15–20 mg/kg IV 8–12-hourly) before imaging, as delay increases risk of permanent vision loss, cavernous sinus thrombosis, and meningitis.
High-YieldNEET PG
Do NOT delay antibiotics while waiting for imaging or culture results. Blood cultures should be drawn, but results take 24–48 hours. Imaging (CT or MRI) is essential to:
Orbital abscess (loculated collection) occurs in ~10–15% of cases and requires surgical drainage in addition to antibiotics. Imaging guides this decision, but antibiotics must not be withheld pending imaging.
Warning
Lumbar puncture is contraindicated in suspected orbital cellulitis until imaging excludes mass effect and raised intracranial pressure. Meningitis is a complication, not a prerequisite for diagnosis.
Antibiotic Coverage
Ceftriaxone covers most aerobic gram-positive and gram-negative organisms; vancomycin covers MRSA and penicillin-resistant pneumococci. Once culture results are available (48–72 hours), de-escalate if appropriate.
Duration
IV antibiotics: 2–4 weeks (depending on response)
Followed by oral antibiotics: 2–4 weeks
Total: 4–8 weeks
Adjunctive Measures
Elevation of head of bed
Topical antibiotics for associated conjunctivitis
NSAIDs for pain and inflammation (not first-line)
Treat underlying sinusitis (may require ENT consultation and imaging-guided drainage)
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.