This patient has orbital cellulitis with clinical improvement on appropriate IV antibiotics, but persistent fever and new/worsening headache raise concern for a serious complication: cavernous sinus thrombosis (CVT) or occult abscess. Despite initial imaging showing no abscess, complications can develop during treatment.
| Complication | Clinical Features | Imaging Findings | Management |
|---|---|---|---|
| Cavernous sinus thrombosis | Bilateral signs, headache, altered mental status, seizures | Contrast-enhanced MRI: filling defect in cavernous sinus | Continue/escalate IV antibiotics, consider anticoagulation |
| Orbital abscess | Failure to improve, localized pain, proptosis plateau | CT/MRI: loculated collection | IV antibiotics + surgical drainage |
| Meningitis | Headache, neck stiffness, photophobia, altered sensorium | CSF pleocytosis, elevated protein | IV antibiotics + lumbar puncture after imaging |
| Inadequate source control | Persistent sinusitis signs | Imaging: active sinusitis, fluid levels | ENT consultation, possible sinus drainage |
Imaging (contrast-enhanced MRI with venography) is more sensitive than lumbar puncture for detecting CVT.
The organism (S. pneumoniae) is sensitive to cephalosporins, so ceftriaxone monotherapy is reasonable after complications are excluded and clinical improvement is documented. However, vancomycin should be continued until imaging excludes CVT and lumbar puncture (if performed) excludes meningitis.
Loading illustration…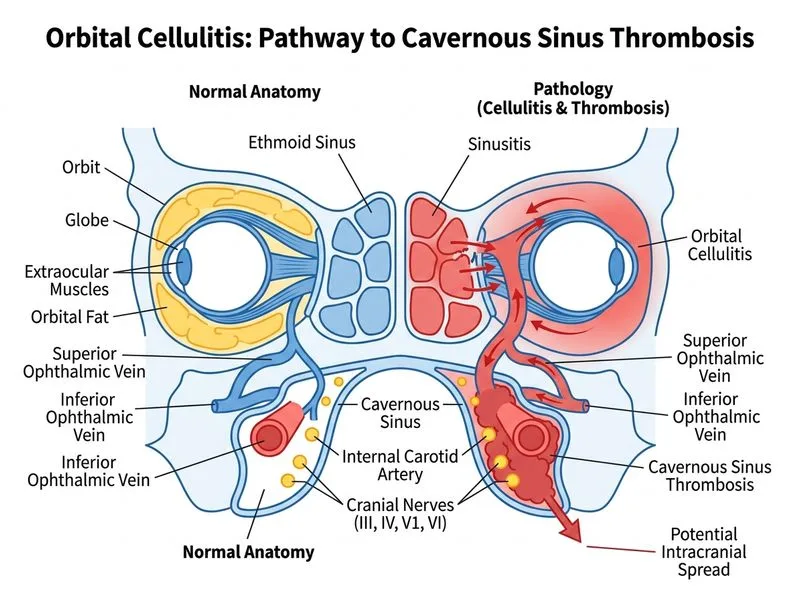
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →