A 28-year-old Indian male presents to the emergency department with acute haemolytic anaemia following consumption of fava beans at a wedding feast. Laboratory investigations reveal: Hb 7.2 g/dL, reticulocyte count 8%, indirect bilirubin 4.2 mg/dL, and LDH 1200 U/L. Peripheral blood smear shows bite cells and Heinz bodies. Urine dipstick is positive for blood but RBCs are absent. Which enzyme deficiency is most likely responsible for this clinical presentation?
A. Glucose-6-phosphatase
B. Transketolase
C. Glucose-6-phosphate dehydrogenase
D. 6-phosphogluconate dehydrogenase
Explanation
Clinical Diagnosis: G6PD Deficiency
Pathophysiology of the Presentation
Key Point
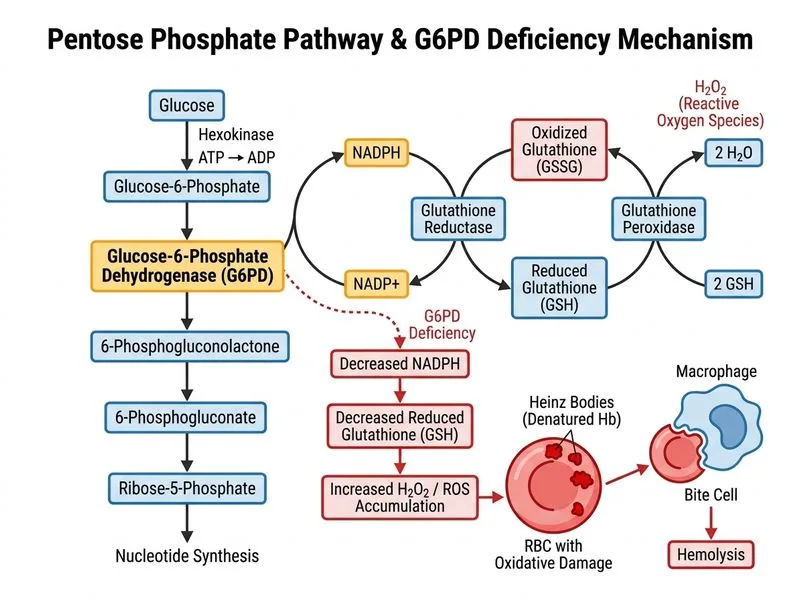
Glucose-6-phosphate dehydrogenase (G6PD) deficiency causes acute haemolytic crises triggered by oxidative stress from fava beans, infections, or certain drugs.
G6PD catalyzes the first committed step of the pentose phosphate pathway (PPP), generating NADPH:
Reducing glutathione (GSSG → 2 GSH) via glutathione reductase
2.
Maintaining reduced glutathione (GSH) pools
3.
Protecting RBCs from oxidative damage
High-YieldNEET PG
Without adequate NADPH, RBCs cannot regenerate GSH, leading to accumulation of reactive oxygen species (ROS) that denature haemoglobin and damage the RBC membrane.
Why This Case Fits G6PD Deficiency
Table
Finding
Mechanism
Acute haemolysis after fava beans
Fava bean oxidants (divicine, isouramil) trigger ROS in G6PD-deficient cells
Denatured haemoglobin polymers from oxidative damage
Positive urine dipstick, no RBCs
Free haemoglobin in urine (haemoglobinuria) from intravascular haemolysis
High reticulocyte count
Bone marrow compensatory response to acute RBC loss
Elevated LDH & indirect bilirubin
Markers of intravascular haemolysis
Clinical Pearl
G6PD deficiency is X-linked recessive; males are predominantly affected. It is the most common enzymatic RBC disorder worldwide, particularly in Mediterranean, African, and Asian populations.
Do not confuse G6PD deficiency with other causes of haemolytic anaemia (hereditary spherocytosis, autoimmune haemolytic anaemia, sickle cell disease). The trigger (fava beans), the presence of Heinz bodies and bite cells, and the X-linked inheritance pattern are pathognomonic for G6PD.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.