A 28-year-old male presents with recurrent infections, jaundice, and dark urine after consuming fava beans. Clinical examination reveals splenomegaly. Hemoglobin is 9.2 g/dL with reticulocytosis. Which investigation is most appropriate to confirm the underlying enzymatic defect in the pentose phosphate pathway?
A. Hemoglobin electrophoresis
B. Peripheral blood smear for Heinz bodies
C. Bone marrow biopsy for erythroid hyperplasia
D. Serum glucose-6-phosphate dehydrogenase (G6PD) activity assay
Explanation
Diagnosis: G6PD Deficiency
Key Point
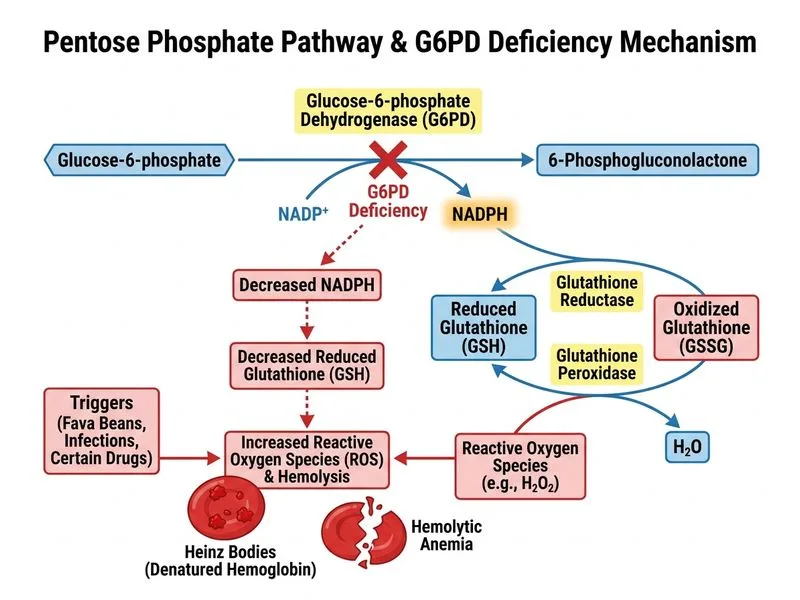
G6PD deficiency is the most common enzyme defect of the pentose phosphate pathway (PPP), affecting ~400 million people worldwide. The clinical presentation of hemolytic anemia triggered by oxidative stress (fava beans, infections, sulfonamides) is pathognomonic.
Why G6PD Activity Assay is Diagnostic
G6PD catalyzes the first committed step of the PPP:
Glucose-6-phosphateG6PD6-phosphogluconolactone
This reaction generates NADPH, which is essential for:
Glutathione reduction (antioxidant defense)
Protection against oxidative stress in RBCs
High-YieldNEET PG
Direct measurement of G6PD enzyme activity in RBCs is the gold standard confirmatory test. It quantifies the enzymatic deficiency and correlates with clinical severity.
Pentose Phosphate Pathway Context
Table
Enzyme
Function
Deficiency Consequence
G6PD
Generates NADPH
↓ Glutathione reduction → oxidative hemolysis
6-PGD
Continues NADPH generation
Rare; milder phenotype
TK (Transketolase)
Non-oxidative phase
Wernicke-Korsakoff (thiamine deficiency)
Clinical Pearl
G6PD activity is often falsely normal during acute hemolytic episodes (young RBCs with higher enzyme levels predominate). Retest 2–4 weeks after recovery for accurate diagnosis.
Mnemonic
NADPH — the critical product of PPP. G6PD deficiency → ↓ NADPH → ↓ reduced glutathione → RBC oxidative damage.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.