A 3-year-old boy from Kerala presents with acute hemolytic anemia, jaundice, and dark urine following consumption of fava beans. Peripheral blood smear shows bite cells and Heinz bodies. G6PD deficiency is suspected. What is the most appropriate immediate next step in management?
A. Start oral folic acid supplementation and discharge home with dietary counseling
B. Measure erythrocyte G6PD enzyme activity level
C. Perform bone marrow aspiration to assess erythropoietic response
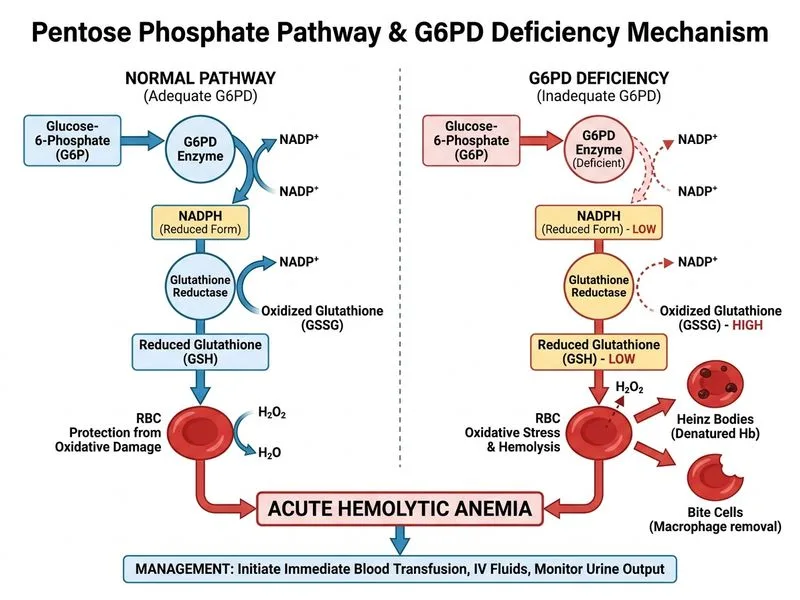
D. Initiate immediate blood transfusion and supportive care with IV fluids and monitoring of urine output
Explanation
Clinical Context
This is a classic presentation of acute hemolytic crisis in G6PD deficiency triggered by oxidative stress from fava bean consumption. The clinical findings (bite cells, Heinz bodies, hemoglobinuria) confirm acute intravascular hemolysis.
Immediate Management Priority
Key Point
In acute hemolytic crisis, the immediate focus is stabilization and prevention of complications, not diagnostic confirmation.
High-YieldNEET PG
The management hierarchy in acute hemolysis:
1.
Immediate: Supportive care (IV fluids, transfusion if needed)
2.
Concurrent: Monitor for complications (acute kidney injury, hyperkalemia)
3.
Later: Enzyme assay confirmation (done during stable phase, not acute crisis)
Why This Approach?
Loading diagram...
Clinical Pearl
G6PD enzyme levels are falsely normal during acute hemolysis (reticulocytosis with high enzyme content). Testing must be deferred 4–6 weeks after crisis resolution for accurate diagnosis.
Key Point
Dark urine indicates myoglobinuria/hemoglobinuria → risk of acute tubular necrosis. Aggressive hydration with urine alkalinization (sodium bicarbonate) prevents precipitation in renal tubules.
Supportive Care Details
IV fluids: 200–300 mL/kg/day to maintain urine output > 200 mL/m²/day
Transfusion: if Hb < 7 g/dL or symptomatic (dyspnea, altered mental status)
Avoid NSAIDs, sulfonamides, antimalarials during recovery