A 48-year-old woman from Mumbai on aspirin 75 mg daily for secondary prevention after a stroke 2 years ago presents with epigastric pain and vomiting for 1 week. Upper endoscopy shows a 2 cm gastric ulcer with active bleeding (Forrest IIb). Rapid urease test is negative. What is the most appropriate next step in management?
A. Stop aspirin, perform endoscopic hemostasis (injection or cautery), and start omeprazole 40 mg BD; restart aspirin after 7 days with gastroprotection
B. Perform angiographic embolization as endoscopy is contraindicated in antiplatelet users
C. Continue aspirin, perform endoscopic hemostasis (injection or cautery), and start omeprazole 40 mg BD plus high-dose H2-blocker
D. Stop aspirin immediately and start omeprazole 40 mg BD; endoscopic hemostasis not needed as she is on antiplatelet therapy
Explanation
Clinical Scenario Analysis
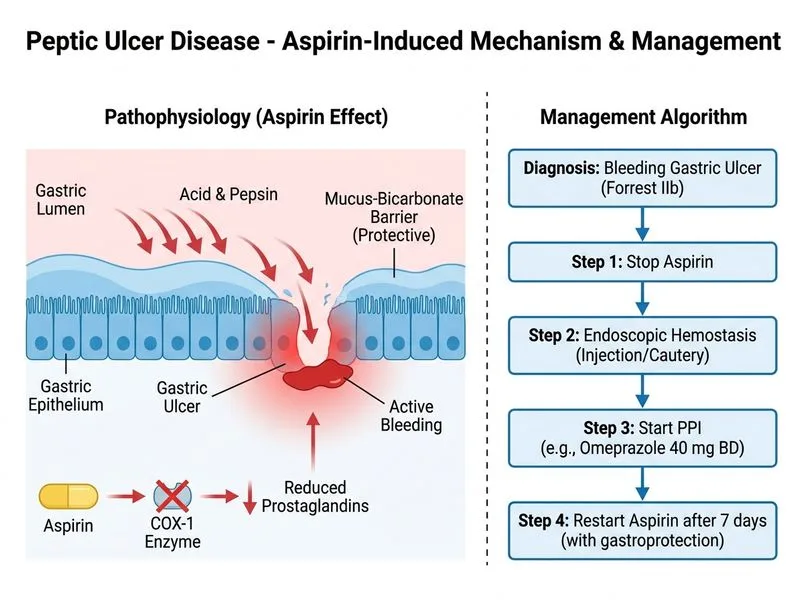
This patient has NSAID-induced (aspirin) peptic ulcer with active bleeding (Forrest IIb). The key challenge is balancing hemostasis with the need to maintain antiplatelet therapy for secondary stroke prevention.
Management Algorithm for Bleeding PUD in Antiplatelet Users
Loading diagram...
Key Point:
Endoscopic hemostasis is the standard of care for bleeding PUD, regardless of antiplatelet therapy status Harrison 21e Ch 297. The presence of active bleeding (Forrest IIb) mandates intervention.
High-Yield: Forrest Classification
Table
Grade
Appearance
Rebleeding Risk
Intervention
Ia
Spurting arterial bleeding
90%
Endoscopic
Ib
Oozing bleeding
80%
Endoscopic
IIa
Visible vessel (no bleeding)
50%
Endoscopic
IIb
Adherent clot
30%
Consider endoscopic
IIc
Flat pigmented spot
10%
Supportive care
III
Clean base
5%
Supportive care
This patient has Forrest IIb → endoscopic hemostasis indicated.
Management of Antiplatelet Therapy During Bleeding
Temporary Cessation Strategy (Preferred for Secondary Prevention)
1.
Stop aspirin temporarily (5–7 days) to allow hemostasis and ulcer stabilization.
2.
Perform endoscopic hemostasis (injection of epinephrine + sclerotherapy, or thermal cautery).
3.
Start PPI 40 mg BD immediately (high-dose for 4–8 weeks).
4.
Restart aspirin after 5–7 days once bleeding has stopped and ulcer is stable, WITH gastroprotection (continue PPI).
Rationale
Aspirin increases bleeding risk by 2–3 fold in PUD.
Temporary cessation (5–7 days) allows clot formation and hemostasis without significantly increasing thrombotic risk in secondary prevention (stroke risk is ~1–2% per week).
Restarting aspirin + PPI reduces rebleeding to <5%.
Clinical Pearl:
H. pylori-negative, NSAID-induced ulcer: This patient is H. pylori-negative, so the ulcer is aspirin-induced. Management focuses on:
1.
Stopping the offending agent (aspirin temporarily).
2.
Hemostasis (endoscopic).
3.
PPI therapy (high-dose).
4.
Restart with gastroprotection (PPI).
Why This Approach?
1.
Endoscopic hemostasis is evidence-based: Reduces rebleeding by 70% and mortality by 30% compared to medical management alone.
2.
Temporary aspirin cessation is safe: 5–7 days of cessation does not significantly increase stroke risk in secondary prevention.
3.
PPI + aspirin restart reduces rebleeding: Combination therapy reduces rebleeding to <5% vs. 20–30% with aspirin alone.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.