## Clinical Diagnosis: Acute Limb Ischemia ### Key Features Pointing to **Acute Embolism** **High-Yield:** The **sudden onset** (2 hours) in a patient with **no prior claudication history** and **intact motor/sensory function** (no sensory loss yet) strongly suggests **acute arterial embolism** rather than acute thrombosis on chronic PAD. **Clinical Pearl:** Acute embolism typically presents with the **6 P's**: 1. **Pain** (sudden, severe) 2. **Pallor** (mottled, pale foot) 3. **Pulselessness** (absent distal pulses) 4. **Paresthesia** (may develop later) 5. **Paralysis** (late finding; indicates irreversible ischemia) 6. **Poikilothermia** (cold limb) In this case, the patient has pain, pallor, pulselessness, and poikilothermia **within 2 hours** — classic acute embolism timeline. ### Acute Arterial Occlusion: Embolism vs. Thrombosis | Feature | **Acute Embolism** | **Acute Thrombosis** | |---|---|---| | **Onset** | Sudden (minutes to hours) | Gradual or sudden | | **Prior claudication** | Absent | Often present | | **Cardiac source** | AF, MI, endocarditis, prosthetic valve | No | | **Limb appearance** | Pale, mottled, cold | May have collaterals | | **Contralateral pulses** | Normal | Often abnormal | | **Management** | **Thromboembolectomy** (surgical) | Thrombolysis or PTA | | **Ischemia time** | <6 hrs: salvageable; >12 hrs: irreversible | Variable | **Key Point:** This patient likely has **atrial fibrillation** (unmentioned but common source) or recent MI. The **absence of prior claudication** and **acute presentation** favor embolism. ## Management Algorithm for Acute Limb Ischemia ```mermaid flowchart TD A[Acute Limb Ischemia<br/>Sudden onset, pulseless]:::outcome --> B{Time since onset?}:::decision B -->|< 6 hours| C{Viable limb?}:::decision B -->|6-12 hours| D{Viable limb?}:::decision B -->|> 12 hours| E[Likely irreversible<br/>Consider amputation]:::urgent C -->|Yes| F{Embolism or<br/>thrombosis?}:::decision D -->|Yes| F F -->|Embolism<br/>Sudden, no prior PAD| G[Immediate Thromboembolectomy]:::action F -->|Thrombosis<br/>Prior claudication| H[Angiography + Thrombolysis/PTA]:::action C -->|No| I[Amputation]:::urgent D -->|No| I G --> J[Reperfusion<br/>Limb salvage]:::outcome H --> K[Reperfusion or<br/>Bypass if needed]:::outcome ``` ## Why Thromboembolectomy Is Correct 1. **Time-critical emergency**: Acute embolism requires **immediate surgical removal** of the thrombus within 6 hours to prevent irreversible tissue damage. 2. **Surgical approach is fastest**: Fogarty catheter thromboembolectomy can be performed under local anesthesia in the OR within minutes, restoring flow before ischemia becomes irreversible. 3. **Thrombolysis is slower**: IV thrombolytics (tPA, urokinase) take 4–24 hours to dissolve the clot — too slow for acute embolism with viable limb at risk. 4. **Angiography delays definitive treatment**: While diagnostic, angiography adds 30–60 minutes; in acute embolism, the diagnosis is clinical and thromboembolectomy should not be delayed. **Warning:** Sensory and motor function are **still intact** — this indicates the limb is still viable. Once paralysis or sensory loss develops, irreversible damage is occurring, and the window for salvage is closing. [cite:Harrison 21e Ch 297; Sabiston Textbook of Surgery Ch 63] 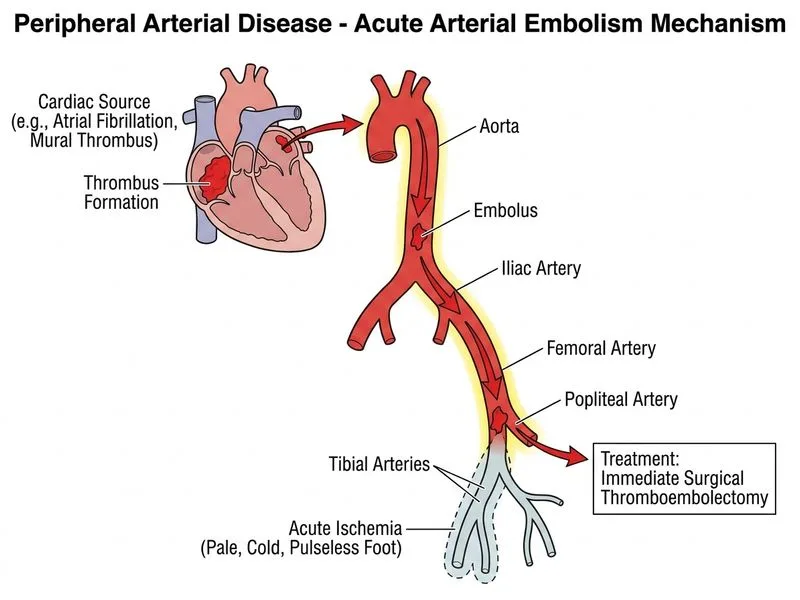
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.