## Management of Claudication in Peripheral Arterial Disease ### Clinical Scenario Analysis This patient presents with **intermittent claudication** (pain with walking, relief with rest) and an ABI of 0.45, confirming significant PAD. The absence of rest pain, tissue loss, or gangrene indicates **stable chronic PAD**, not acute limb-threatening ischemia. ### First-Line Management Strategy **Key Point:** Claudication management is **primarily medical and lifestyle-based** unless there is acute limb threat or failed conservative therapy. The cornerstone of treatment includes: | Component | Rationale | |-----------|----------| | **Antiplatelet therapy** (Aspirin 75 mg OD) | Reduces cardiovascular events and mortality | | **Cilostazol 100 mg BD** | Phosphodiesterase-3 inhibitor; improves claudication distance by 25–50% | | **Smoking cessation** | Most critical modifiable risk factor; halts disease progression | | **Supervised exercise** (6–12 weeks) | Improves walking distance through collateral formation and metabolic adaptation | | **Statin therapy** | Stabilizes plaque, reduces CV events | **High-Yield:** Cilostazol is contraindicated in heart failure (reduces ejection fraction) but is first-line for claudication in PAD. ### When to Revascularize Revascularization (PTA, stenting, or surgery) is reserved for: - Failed conservative therapy (after 3–6 months) - Critical limb ischemia (rest pain, tissue loss, ABI < 0.4 with symptoms) - Acute limb ischemia This patient is **not yet a candidate** for intervention; he requires optimized medical therapy first. ### Why Other Options Are Incorrect **Amputation:** Reserved for irreversible tissue loss, gangrene, or failed revascularization. Premature amputation is a surgical error in stable claudication. **Anticoagulation (heparin/warfarin):** Indicated for acute thrombotic occlusion or embolic disease, not chronic stenosis. No role in stable PAD. **Immediate angiography/PTA:** The question states the patient is "not a candidate for revascularization," which typically implies anatomical unsuitability, severe comorbidity, or failure to complete conservative therapy first. **Clinical Pearl:** Supervised exercise programs increase claudication-free walking distance by up to 150% and should always precede intervention in stable disease [cite:Harrison 21e Ch 243]. 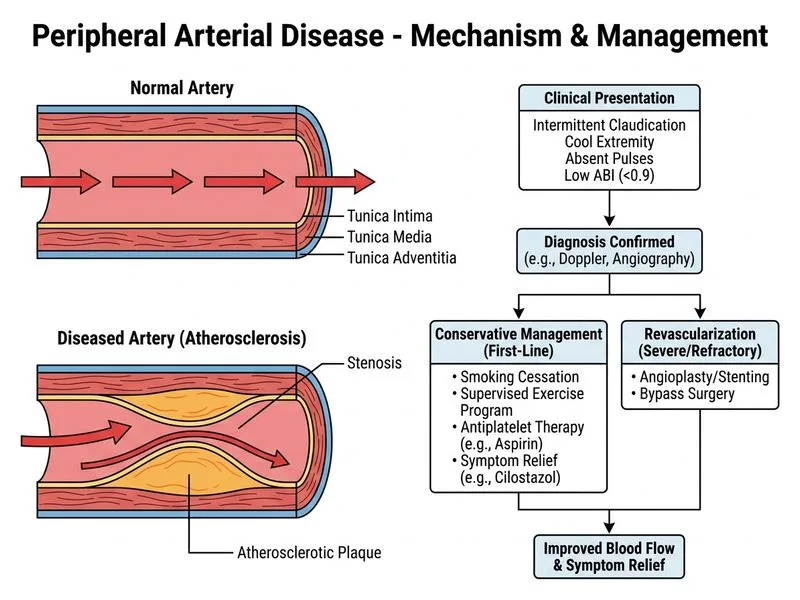
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.