A 35-year-old man with known chronic obstructive pulmonary disease presents with acute dyspnea and chest pain. Chest X-ray in the upright position shows a small right pneumothorax with a visceral pleural line 2 cm from the chest wall. The patient is hemodynamically stable with oxygen saturation 94% on room air. However, the clinician is concerned about missing a small pneumothorax on the contralateral side. Which imaging modality provides the HIGHEST sensitivity for detecting occult or small bilateral pneumothorax?
A. Ultrasound of the chest with assessment for the 'barcode sign' and absence of lung sliding
B. High-resolution CT chest in both inspiration and expiration
C. Decubitus chest X-ray with the left side dependent
D. Repeat upright posteroanterior and lateral chest X-rays with inspiration and expiration films
Explanation
Imaging Modalities for Occult Pneumothorax Detection
Sensitivity Comparison Across Modalities
Table
Modality
Sensitivity for Small PTX
Sensitivity for Bilateral PTX
Advantages
Limitations
Upright CXR (PA/Lateral)
60–90%
Moderate (may miss small contralateral)
Readily available, low cost
Limited for small PTX, poor for supine patients
Expiration CXR
Improved vs. inspiration
Better than inspiration alone
Increases PTX visibility
Still misses ~10–15% of small PTX
Decubitus CXR
70–85%
Moderate
Useful for supine patients
Less sensitive than CT
High-resolution CT (HRCT)
95–100%
95–100%
Gold standard; detects 1–2 mm PTX
Higher radiation dose; not first-line for stable patients
High-resolution CT with thin-section slices (1–2 mm) in both inspiration and expiration can detect pneumothorax as small as 1–2 mm, making it the gold standard for:
Occult (clinically suspected but radiographically occult) pneumothorax
Small bilateral pneumothorax
Pneumothorax in supine or obese patients
Assessment of underlying lung disease (bullae, blebs)
Detects tiny air collections — even 1–2 mm of air is visible
3.
Bilateral assessment — entire thorax is imaged simultaneously
4.
Characterizes underlying lung — can identify COPD, bullae, or fibrosis predisposing to recurrence
Clinical Decision-Making Algorithm
Loading diagram...
Why Other Options Are Suboptimal
Clinical Pearl
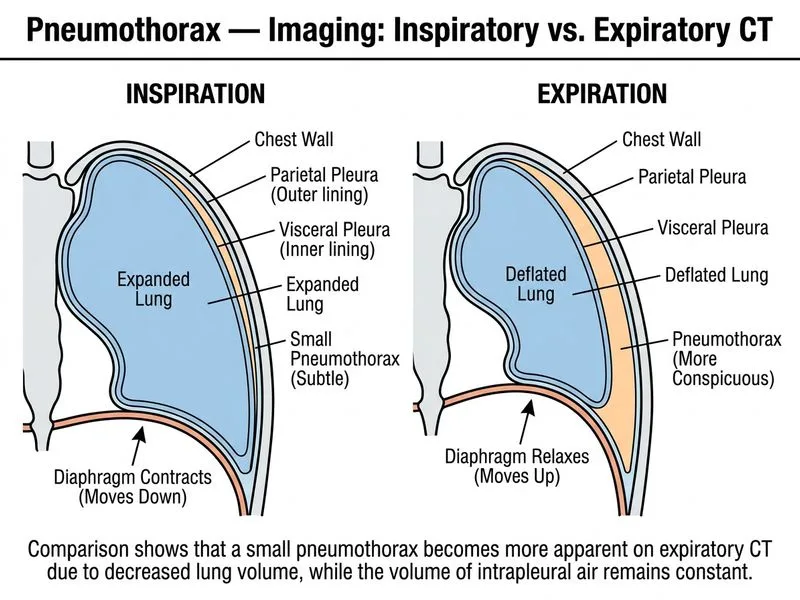
Expiration films increase the relative size of pneumothorax (lung volume decreases, PTX volume stays constant), improving visibility on radiographs. However, even with expiration films, sensitivity for small bilateral PTX remains 85–90%, missing ~10–15% of cases. CT is definitively superior.
Mnemonic: "CT Beats All" for Occult PTX
Cross-sectional imaging
Thin slices detect 1–2 mm air
Bilateral assessment in one study
Excels in supine/obese patients
Accurate for underlying lung disease
True gold standard
Sensitivity >95%
Tip
In a stable patient with clinical suspicion of bilateral pneumothorax, HRCT is justified because it:
Definitively rules in/out contralateral PTX
Characterizes underlying COPD severity
Guides management (observation vs. intervention)
Prevents missed diagnosis and complications
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.