A 35-year-old male smoker with known COPD presents with acute dyspnea. Chest X-ray shows a small right-sided pneumothorax (< 2 cm at the hilum). The patient is clinically stable with oxygen saturation 94% on room air. Which investigation is most appropriate to assess the need for intervention and guide management?
A. Ventilation-perfusion (V/Q) scan
B. Repeat CXR at 2–4 weeks to assess progression
C. CT chest with volumetric measurement of pneumothorax
D. Arterial blood gas analysis
Explanation
Assessment of Pneumothorax in COPD: Role of ABG
Clinical Context
This patient has a secondary spontaneous pneumothorax (SSP) — occurring in the setting of known COPD. SSP is clinically more dangerous than primary spontaneous pneumothorax (PSP) because the underlying lung disease reduces physiological reserve. Even a "small" pneumothorax (< 2 cm at the hilum on CXR) can cause significant respiratory compromise in a COPD patient.
Investigation of Choice: Arterial Blood Gas (ABG) Analysis
Key Point
In a patient with COPD and a secondary spontaneous pneumothorax, ABG analysis is the most appropriate investigation to assess the need for intervention and guide management. It directly quantifies the physiological impact of the pneumothorax on gas exchange and ventilation.
High-YieldNEET PG
The British Thoracic Society (BTS) 2010 Guidelines on Spontaneous Pneumothorax explicitly state that in secondary spontaneous pneumothorax, ABG should be performed to assess:
Per BTS guidelines, even a "small" SSP (< 2 cm on CXR) in a symptomatic patient with COPD should be admitted and considered for intervention — unlike PSP where conservative management is acceptable. ABG findings of hypoxaemia or hypercapnia mandate active intervention (aspiration or chest drain), regardless of radiological size.
Why ABG Guides Management Here
Table
Parameter
Significance in SSP
PaO₂ < 8 kPa
Significant hypoxaemia → intervention required
PaCO₂ > 6 kPa
Ventilatory failure → chest drain, not just aspiration
pH < 7.35
Respiratory acidosis → urgent intervention
SpO₂ 94% on room air
Already borderline — ABG needed to confirm true oxygenation status
Why the Other Options Are Less Appropriate
Option A (Repeat CXR at 2–4 weeks): Appropriate follow-up for small primary spontaneous pneumothorax managed conservatively — NOT for SSP in COPD, where early intervention is often needed.
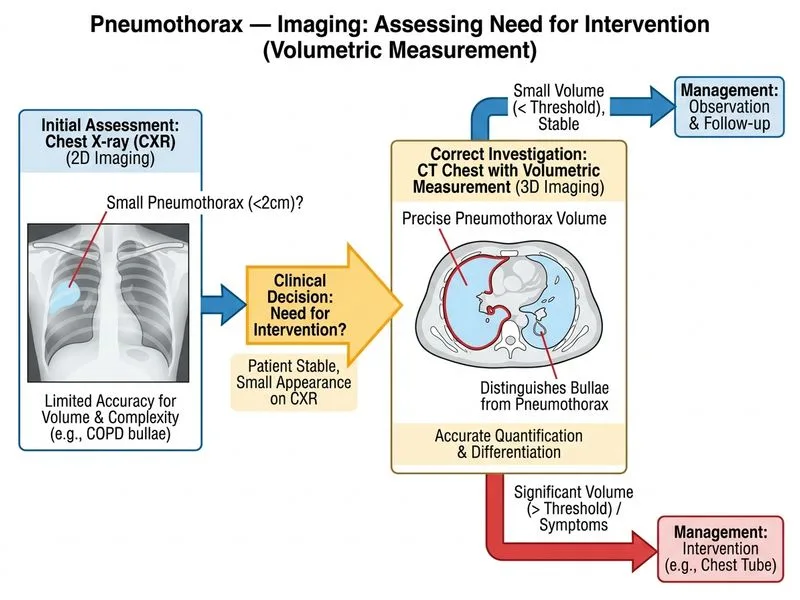
Option B (CT chest with volumetric measurement): CT is useful for assessing underlying bullae/blebs and recurrence risk, but it is not the immediate investigation to guide the need for intervention in an acute setting. BTS guidelines do not recommend routine CT for initial management decisions in SSP.
Option D (V/Q scan): Indicated for suspected pulmonary embolism, not for pneumothorax management.
Key Point
The question asks what investigation is most appropriate to assess the need for intervention and guide management — this is a physiological question answered by ABG, not an anatomical/volumetric question answered by CT.
BTS Guidelines for the Management of Spontaneous Pneumothorax, Thorax 2010; Harrison's Principles of Internal Medicine, 21st ed.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.