| Feature | Primary Spontaneous | Secondary |
|---|---|---|
| Underlying lung disease | No | Yes (COPD, CF, ILD, malignancy) |
| Small PTX (≤2 cm) | Conservative: O₂ + observation | Consider intervention |
| Large PTX (>2 cm) | Intervention if symptomatic | Always intervene |
| Recurrence rate | 20–30% | 40–50% |
| Mortality risk | Low | Higher |
Loading illustration…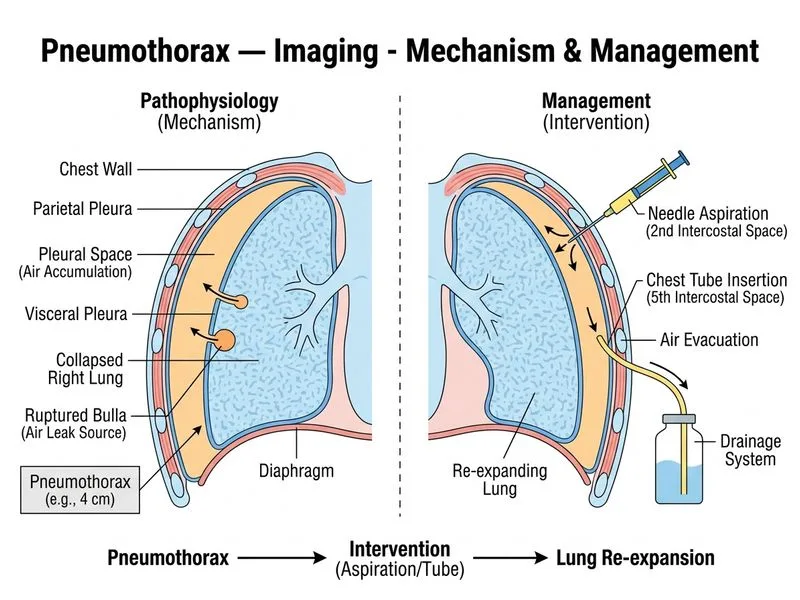
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →