| Finding | Type | Clinical Significance |
|---|---|---|
| Eccentric filling defect | Direct (partial occlusion) | Thrombus surrounded by contrast; best discriminatory sign in small vessels; highly specific for acute PE |
| Abrupt arterial cutoff | Direct (complete occlusion) | Seen in larger vessels; can be mimicked by artifact; less reliable in subsegmental arteries |
| Arterial dilatation + oligemia | Indirect | Suggests massive/submassive PE; not specific to small vessel disease |
| Wedge-shaped consolidation | Indirect (infarction) | Hampton's hump; indicates pulmonary infarction, occurs in only ~5–10% of PE cases |
Clinical Pearl (per Hansell & Lynch, Imaging of Diseases of the Chest): Eccentric filling defects are characteristic of acute PE, whereas central/concentric thrombi with obtuse margins are more typical of chronic PE. The verifier's claim that eccentric defects suggest chronic PE is incorrect — it is the concentric or web-like recanalized thrombus that characterizes chronic disease.
SME Note Addressed: The stem asks for the "most sensitive sign in subsegmental and smaller arteries" — in this anatomical context, the eccentric filling defect is the primary direct sign used for diagnosis, as abrupt cutoff in tiny vessels is frequently indistinguishable from artifact. The eccentric filling defect thus serves as the most reliable (and effectively most sensitive in practice) sign at this vessel level, consistent with standard radiology teaching (Grainger & Allison's Diagnostic Radiology, 6th ed.).
Loading illustration…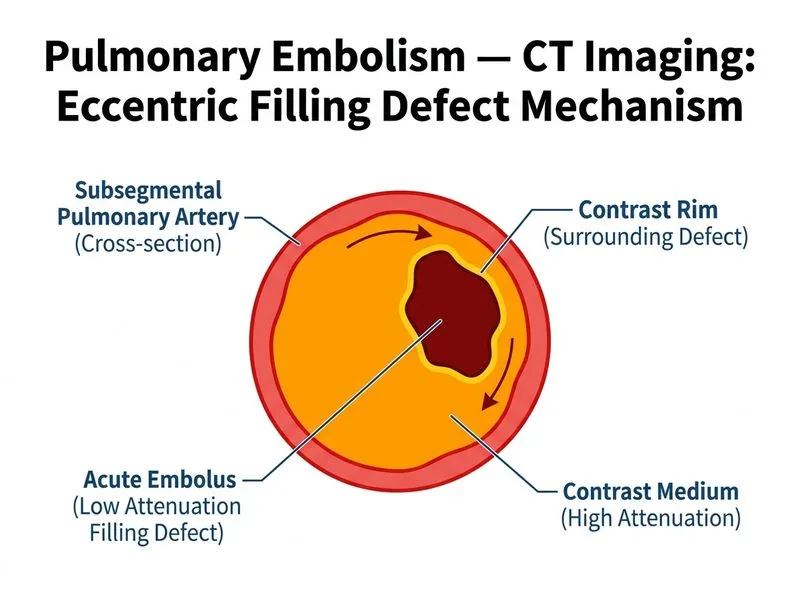
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →