This patient has classic risk factors for venous thromboembolism (recent orthopedic surgery, immobility) and presents with acute dyspnea and pleuritic chest pain—the cardinal symptom of pulmonary infarction.
| Feature | Description | Significance |
|---|---|---|
| Filling defect | Central or eccentric thrombus within pulmonary artery lumen | Direct visualization of embolus |
| Wedge-shaped opacity | Peripheral consolidation, apex pointing centrally (Hampton's hump) | Hemorrhagic infarction |
| Location | Usually lower lobes (gravity-dependent) | PE preferentially lodges distally |
| Pleural base | Consolidation touching pleural surface | Indicates infarction, not just PE |
Pulmonary infarction develops in only ~10% of PEs because the lung has dual blood supply (pulmonary + bronchial arteries). Infarction occurs when:
| Diagnosis | CTPA Finding | Distinguishing Feature |
|---|---|---|
| PE with infarction | Filling defect + wedge opacity | Apex toward hilum; follows vascular distribution |
| Pneumonia | Consolidation only | No filling defect; may be bilateral; air bronchograms |
| Saddle embolus | Large thrombus at PA bifurcation | Bilateral PE; severe RV strain; no wedge opacity required |
Harrison 21e Ch 297
Loading illustration…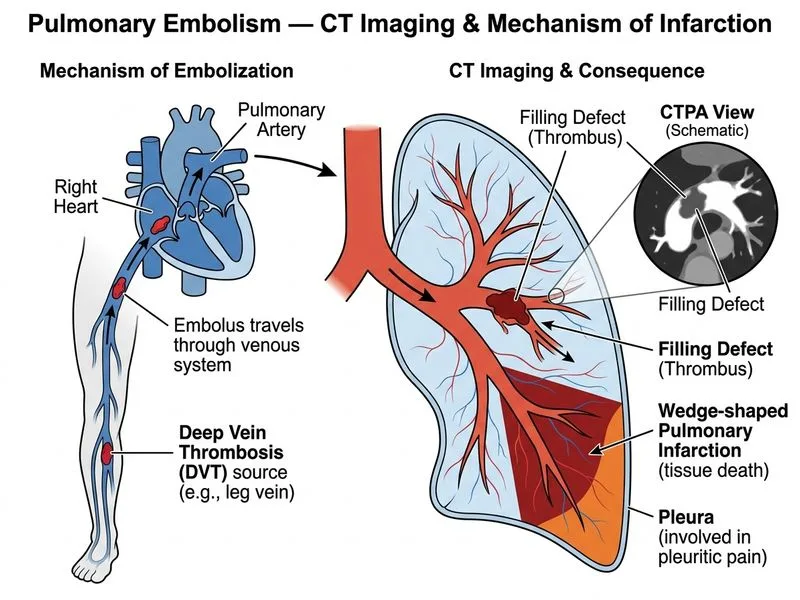
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →