This patient demonstrates hemodynamic instability (syncope, hypotension, shock) with right heart strain (RV dilatation on imaging, ECG changes, elevated troponin). These are hallmarks of massive PE requiring urgent intervention.
| Classification | CTPA Finding | Hemodynamic Status | RV Strain | Management |
|---|---|---|---|---|
| Subsegmental | Filling defect in subsegmental artery only | Stable | Absent | Anticoagulation ± observation |
| Segmental | Filling defect in segmental artery ± multiple segments | Usually stable | May be present | Anticoagulation ± monitoring |
| Lobar | Filling defect in lobar artery | Variable | Often present | Anticoagulation; consider escalation if unstable |
| Massive (Saddle) | Filling defect at PA bifurcation ± bilateral extension | Unstable (shock, syncope) | Severe (RV > 1.5 × LV) | Urgent thrombolysis / embolectomy |
Unlike smaller PEs (which are managed with anticoagulation alone), massive PE has a mortality of 30–50% without intervention and requires immediate thrombolysis (alteplase, tenecteplase) or surgical/catheter embolectomy.
Harrison 21e Ch 297; Chest Radiology: The Essentials Ch 8
Loading illustration…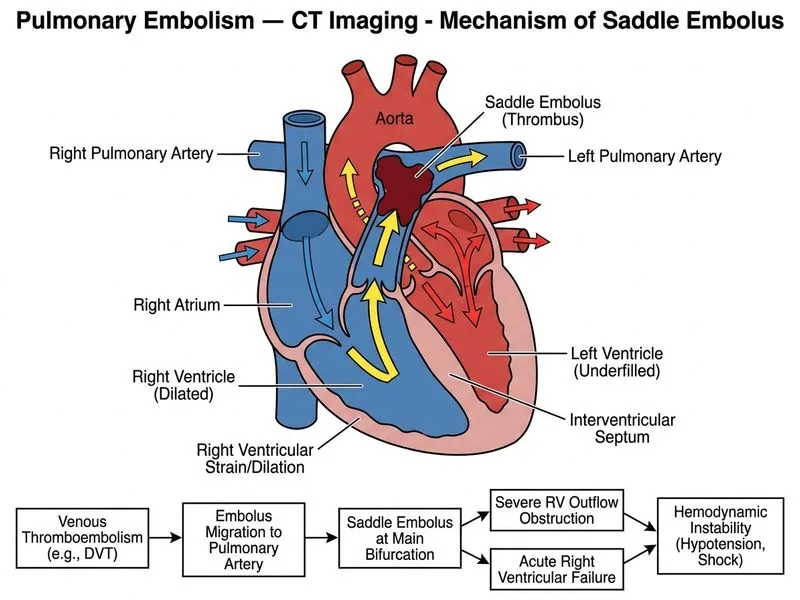
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →