A 58-year-old man with acute onset dyspnea and pleuritic chest pain presents to the emergency department. Clinical suspicion for pulmonary embolism is high. Which imaging modality is the investigation of choice for confirming acute pulmonary embolism?
A. Computed tomography pulmonary angiography (CTPA)
B. Chest X-ray followed by D-dimer
C. Magnetic resonance pulmonary angiography (MRPA)
D. Ventilation-perfusion (V/Q) scan
Explanation
Investigation of Choice for Acute PE
Key Point
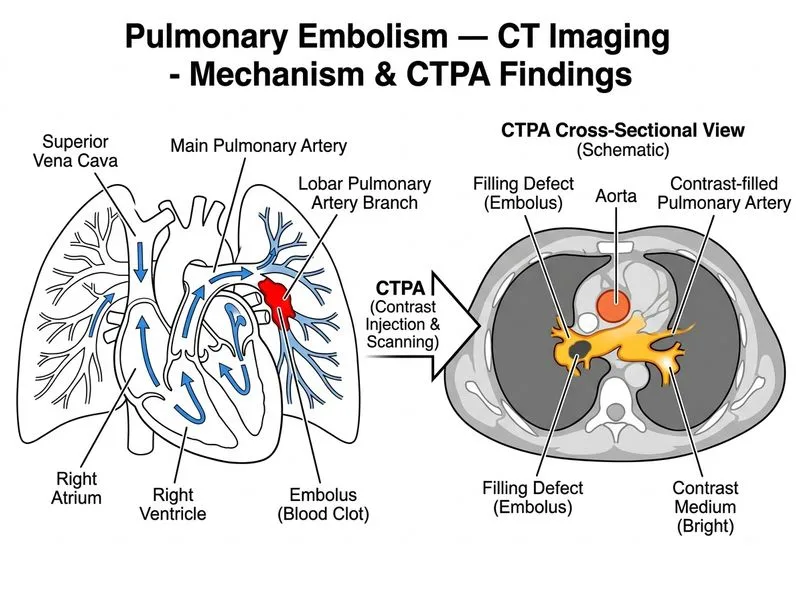
Computed tomography pulmonary angiography (CTPA) is the gold standard and investigation of choice for confirming acute pulmonary embolism in hemodynamically stable patients.
Why CTPA is Superior
High-YieldNEET PG
CTPA offers:
High sensitivity (94–98%) and specificity (95–98%) for central and segmental emboli
Fast acquisition time (< 1 minute)
Ability to visualize alternative diagnoses (pneumonia, aortic dissection, pneumothorax)
Widely available in most hospitals
Can assess right ventricular strain and guide risk stratification
Comparison of Imaging Modalities
Table
Modality
Sensitivity
Specificity
Advantages
Disadvantages
CTPA
94–98%
95–98%
Fast, high accuracy, alternative diagnoses
Radiation, contrast allergy
V/Q Scan
80–90%
80–90%
Lower radiation, no contrast
Slower, high false-positive rate, needs baseline CXR
MRPA
90–95%
95–98%
No radiation, no iodine contrast
Slow, contraindicated with metallic implants, less available
CXR + D-dimer
Variable
Variable
Initial screening
Low specificity, not diagnostic
Clinical Pearl
CTPA is preferred in hemodynamically stable patients with intermediate to high clinical probability. In patients with renal insufficiency or contrast allergy, MRPA or V/Q scan may be alternatives.
Role of D-dimer
Key Point
D-dimer is a screening tool with high sensitivity but low specificity. A negative D-dimer in low-risk patients can exclude PE without imaging; however, it cannot diagnose PE and must always be followed by imaging in intermediate/high-risk patients.
CTPA Protocol Features
1.
Timing: Bolus tracking or test bolus to optimize pulmonary artery opacification