A 58-year-old man with a 3-day history of acute onset dyspnea and pleuritic chest pain presents to the emergency department. His D-dimer is elevated at 2.5 µg/mL. Chest X-ray shows a small right pleural effusion but no consolidation or pneumothorax. Arterial blood gas reveals mild hypoxemia (PaO₂ 72 mmHg on room air). Clinical suspicion for pulmonary embolism is high. What is the most appropriate next step in management?
A. Start empirical thrombolysis and arrange CTPA within 24 hours
B. Administer therapeutic anticoagulation with unfractionated heparin while awaiting CT pulmonary angiography
C. Obtain CT pulmonary angiography (CTPA) immediately
D. Perform V/Q scan to exclude PE before commencing anticoagulation
Explanation
Clinical Context
This patient has a high pretest probability of PE based on acute dyspnea, pleuritic chest pain, elevated D-dimer, and hypoxemia. The chest X-ray is relatively clear, making it suitable for CTPA imaging.
Why CTPA is the Next Step
Key Point
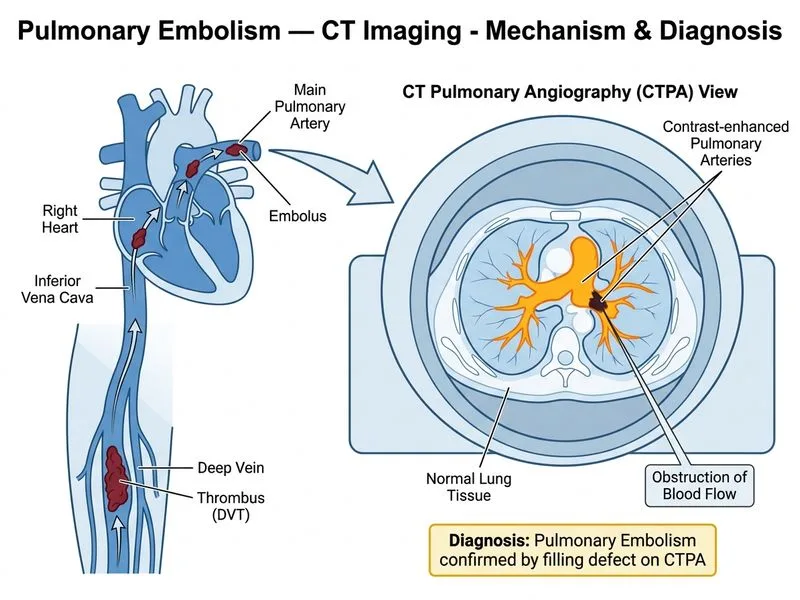
CT pulmonary angiography (CTPA) is the gold standard imaging modality for diagnosis of PE in hemodynamically stable patients with high clinical suspicion and interpretable chest X-rays.
High-YieldNEET PG
CTPA has:
Sensitivity: 83–100% (depending on PE size and technique)
Specificity: >95%
Fast acquisition time (10–15 seconds)
Allows assessment of right heart strain and alternative diagnoses
Management Algorithm
Loading diagram...
Clinical Pearl
Anticoagulation should NOT be delayed awaiting imaging in high-risk patients, but CTPA is performed urgently (not after anticoagulation is started). In this case, the patient is hemodynamically stable, so CTPA is the diagnostic priority.
Tip
Remember the "rule of 90s" — CTPA should be performed within 90 minutes of presentation in suspected PE to guide definitive therapy.
Harrison 21e Ch 297
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.