A 62-year-old woman with a history of recent hip fracture surgery (5 days ago) presents with acute dyspnea and tachycardia. CT pulmonary angiography shows a filling defect in the right lower lobe segmental artery consistent with acute PE. Right ventricular diameter is 4.2 cm (normal <3.5 cm) on the same CT scan, and troponin I is elevated at 0.08 ng/mL. The patient's blood pressure is 128/82 mmHg and heart rate is 112 bpm. What is the most appropriate next step in management?
A. Initiate anticoagulation with low-molecular-weight heparin and observe in the intensive care unit
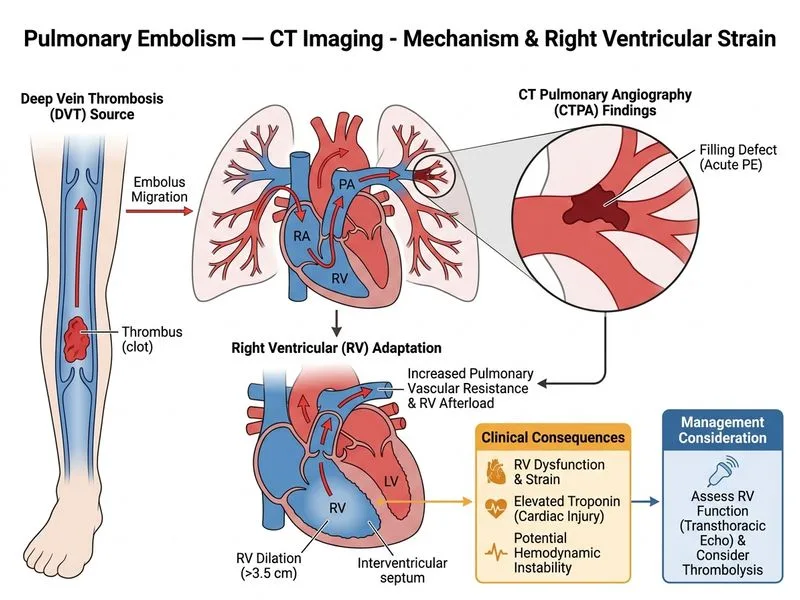
B. Perform bedside transthoracic echocardiography to assess right ventricular function and consider thrombolysis
C. Start empirical thrombolysis immediately without further testing
D. Arrange urgent pulmonary artery catheterization for hemodynamic assessment
Explanation
Clinical Context
This patient has confirmed PE with imaging evidence of right ventricular strain (RV dilation to 4.2 cm, elevated troponin I) but remains hemodynamically stable (BP 128/82 mmHg, no shock/hypotension). This represents intermediate-high risk PE (also called submassive PE per older terminology).
Risk Stratification of PE
Table
Risk Category
Hemodynamics
RV Dysfunction
Biomarkers
Management
Low-risk
Stable
No
Normal
Anticoagulation alone; early discharge
Intermediate-low
Stable
Yes OR elevated biomarkers
Elevated
Anticoagulation + monitoring
Intermediate-high
Stable
Yes AND elevated biomarkers
Elevated
Anticoagulation + echo assessment; rescue thrombolysis if deterioration
High-risk (Massive)
Shock/hypotension
Yes
Elevated
Immediate thrombolysis or embolectomy
Key Point
This patient has BOTH RV dilation on CT AND elevated troponin, placing her in the intermediate-high risk category. The next step is bedside TTE to confirm RV dysfunction and guide escalation decisions — not immediate thrombolysis, which is reserved for hemodynamic deterioration or massive PE.
Why Bedside Echo is the Best Next Step
High-YieldNEET PG
Transthoracic echocardiography in PE evaluates:
RV/LV diameter ratio (>0.9 confirms dysfunction)
RV free wall hypokinesis (McConnell's sign)
Presence of thrombus in transit
Pericardial effusion
Tricuspid regurgitation velocity (estimate PA pressure)
Clinical Pearl
CT-derived RV dilation is a screening tool, but bedside TTE provides real-time functional assessment and is the standard confirmatory step before escalating to thrombolysis in stable patients. ESC 2019 guidelines recommend TTE to confirm RV dysfunction in intermediate-high risk PE before considering reperfusion therapy.
Why the Other Options Are Incorrect
Option A (LMWH + ICU observation alone): While anticoagulation is essential and ICU admission is appropriate, this option omits the critical step of echocardiographic assessment needed to guide potential escalation. Anticoagulation alone without echo-guided monitoring is insufficient for intermediate-high risk PE.
Option C (Pulmonary artery catheterization): Invasive hemodynamic assessment via PA catheter is rarely first-line in modern PE management. It is not recommended as the initial step when non-invasive echo can provide equivalent or superior functional information with less procedural risk.
Option D (Empirical thrombolysis immediately): Thrombolysis carries significant bleeding risk (including intracranial hemorrhage ~1–3%). In a hemodynamically stable patient, immediate thrombolysis without echo confirmation is not indicated. Notably, this patient had hip fracture surgery only 5 days ago — recent major surgery is a relative contraindication to thrombolysis, further supporting a measured approach with echo assessment before any reperfusion decision. Thrombolysis is reserved for massive PE (hemodynamic collapse) or rescue therapy after deterioration on anticoagulation.
The combination of RV dilation (4.2 cm) + elevated troponin in a normotensive patient is the classic intermediate-high risk pattern. Echo is the pivotal next step — it confirms dysfunction and serves as the gatekeeper before any reperfusion decision.
Harrison's Principles of Internal Medicine 21e, Ch. 297; ESC Guidelines on Acute Pulmonary Embolism 2019 (Konstantinides et al., Eur Heart J 2020)
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.