The radial nerve travels in the spiral groove (radial groove) on the posterior surface of the mid-shaft humerus. A fracture at this level causes direct nerve trauma or compression from callus formation.
| Feature | Findings |
|---|---|
| Motor deficit | Wrist drop (loss of wrist extension via ECRB, ECRL, ECU) + thumb IP extension loss (EPL) |
| Sensory loss | Dorsal first web space (radial-supplied area) |
| Nerve branches affected | Both motor (posterior interosseous nerve) and sensory (superficial radial nerve) branches |
| Mechanism | Direct trauma or compression in spiral groove |
The combination of wrist drop (ECRB/ECRL loss), thumb IP extension loss (EPL loss), and dorsal web space sensory loss (superficial radial nerve) indicates injury to the complete radial nerve at the spiral groove level, where both motor and sensory branches are still together.
Clinically Oriented Anatomy Moore 8e Ch 6
Loading illustration…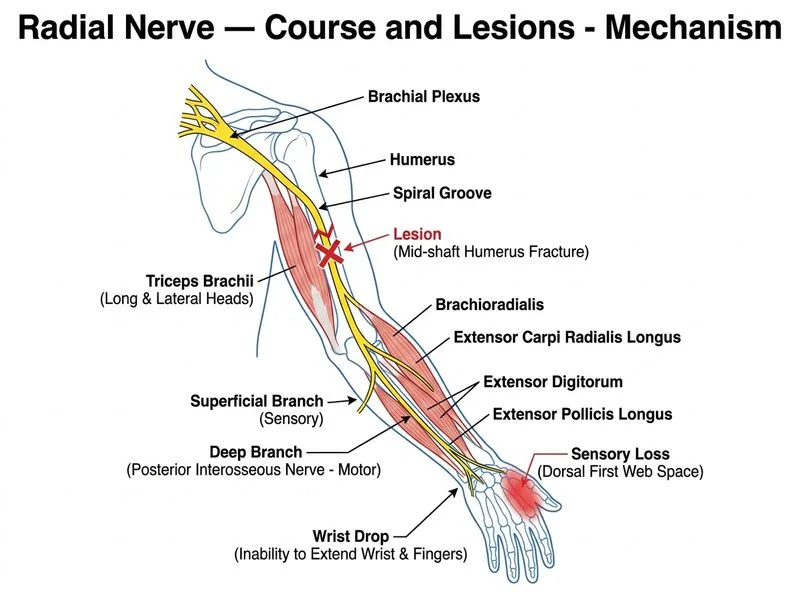
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →