The radial nerve divides into its terminal branches distal to the elbow:
The PIN is particularly vulnerable at the supinator muscle level (just distal to radial head) due to:
| Feature | PIN Injury | Radial Nerve Proper Injury |
|---|---|---|
| Wrist extension | Weak (ECRB, ECRL innervated by PIN) | Weak |
| Finger extension | Weak/absent (EDC, EIP innervated by PIN) | Weak |
| Thumb IP extension | Weak (EPL innervated by PIN) | Weak |
| Thumb opposition | Normal (median nerve) | Normal |
| Dorsal web space sensation | Normal (superficial radial nerve intact) | Absent |
| Palm sensation | Normal (median/ulnar) | Normal |
The patient has motor loss (weak finger and wrist extension) but intact sensation (normal dorsal web space sensation and palm sensation). This dissociation—motor loss without sensory loss—is pathognomonic for PIN injury, which is a pure motor nerve. The radial head fracture-dislocation is the anatomical mechanism: PIN passes through the supinator muscle just distal to the radial head and is vulnerable to compression or traction.
Clinically Oriented Anatomy Moore 8e Ch 6
Loading illustration…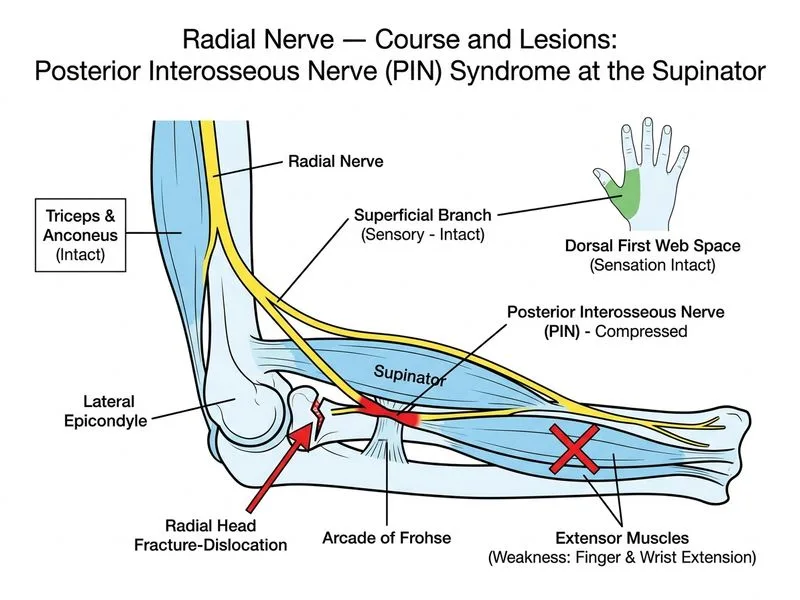
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →