| Time Point | Clinical Status | Electrophysiological Finding | Action |
|---|---|---|---|
| 0–3 weeks | No recovery expected | Conduction block (neuropraxia) or no changes | Observe clinically |
| 3–4 weeks | No clinical recovery | EMG shows denervation potentials | Order EMG/NCS |
| 8 weeks | Persistent deficit | Complete conduction block or no motor units | EMG/NCS needed to classify injury severity |
| 12+ weeks | No recovery | Chronic denervation | Consider surgical intervention |
While spontaneous recovery can occur up to 12 weeks, continuing without electrophysiological assessment is suboptimal. EMG/NCS at 8 weeks provides critical prognostic information and may identify a complete lesion that requires surgical intervention before the "window of opportunity" for nerve repair closes (typically 12–18 months post-injury).
Surgical exploration without EMG/NCS confirmation is premature. If EMG shows neuropraxia or incomplete axonotmesis with some motor recruitment, surgery may not be indicated. Conversely, if EMG shows complete denervation, surgery becomes more justified.
Intravenous immunoglobulin has no role in traumatic peripheral nerve injuries. It may be used in autoimmune neuropathies (e.g., CIDP) but is not indicated here.
Loading illustration…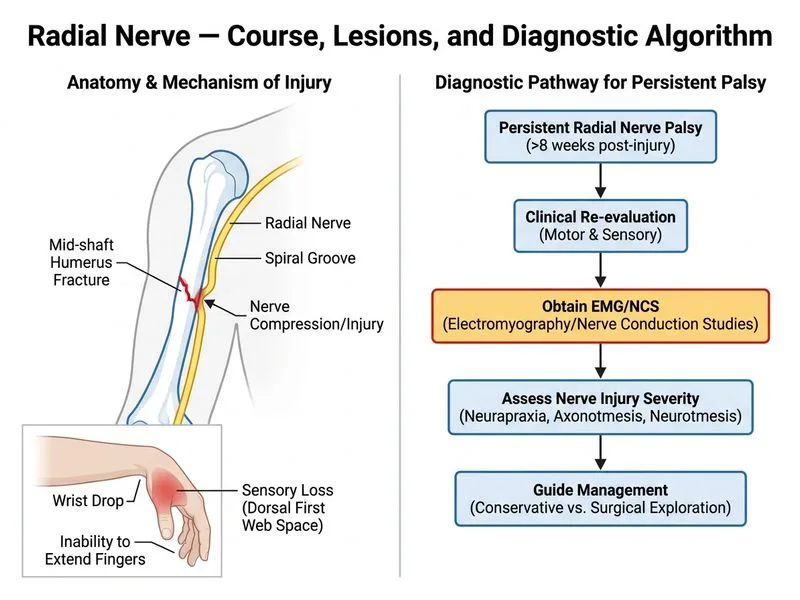
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →