The radial nerve follows a critical anatomical path through the upper limb:
| Feature | Spiral Groove Lesion | Lesion Distal to PIN Origin |
|---|---|---|
| Wrist extension | Lost | Lost (ECRL spared if very distal) |
| Finger extension | Lost | Lost |
| Thumb extension | Lost | Lost |
| Sensation — dorsal 1st web space | Lost | Preserved |
| Sensation — dorsal hand | Lost | Preserved |
A lesion distal to the PIN origin (e.g., posterior interosseous nerve syndrome at the radial tunnel) affects only the motor PIN; the superficial radial nerve is already separate and unaffected → no sensory loss over the dorsal first web space.
Option C ("weakness of finger extension with preserved wrist extension") describes the classic finding of a proximal PIN lesion (e.g., radial tunnel syndrome), not a feature that distinguishes spiral groove from distal-to-PIN lesions. Furthermore, the stem itself already states preserved finger extension, making Option C circular and non-discriminating. Both spiral groove and distal PIN lesions can produce finger extension loss; the sensory status is the reliable localizing feature.
"Spiral = Sensory + Motor lost; PIN-only = Motor lost, Sensation Spared"
Reference: Gray's Anatomy for Students, 4th ed.; Aids to the Examination of the Peripheral Nervous System (Medical Research Council); Netter's Clinical Anatomy.
Loading illustration…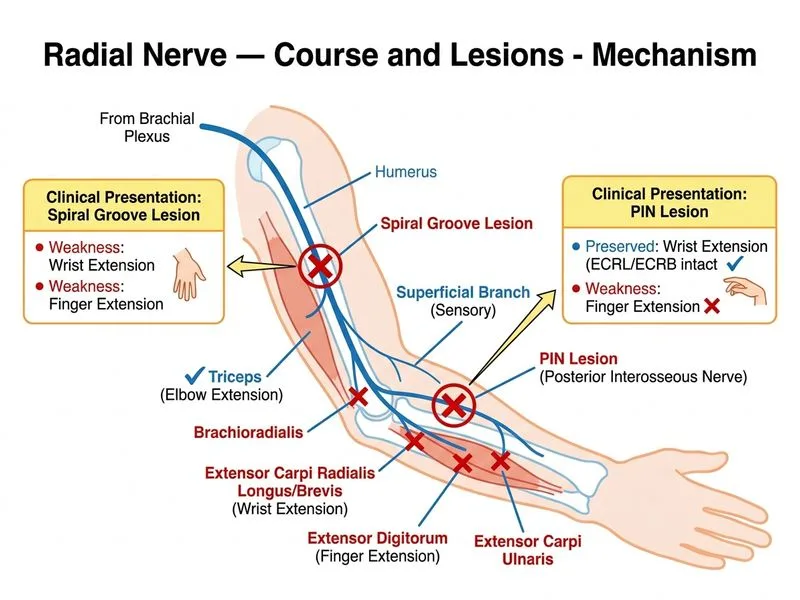
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →