A 62-year-old Indian man with a 15-year history of chronic kidney disease (CKD stage 3b) undergoes routine ultrasound screening. A 3 cm incidental mass is discovered in the left kidney. Core needle biopsy shows cells with abundant clear cytoplasm, well-defined cell borders, and low nuclear grade. The tumor does not invade the renal capsule or blood vessels. Immunohistochemistry is positive for carbonic anhydrase IX (CAIX) and negative for cytokeratin 7. What is the most likely diagnosis and what is the expected 5-year survival rate for this stage?
A. Acquired cystic disease-associated RCC, 5-year survival ~50%
B. Papillary RCC, Stage I, 5-year survival ~80%
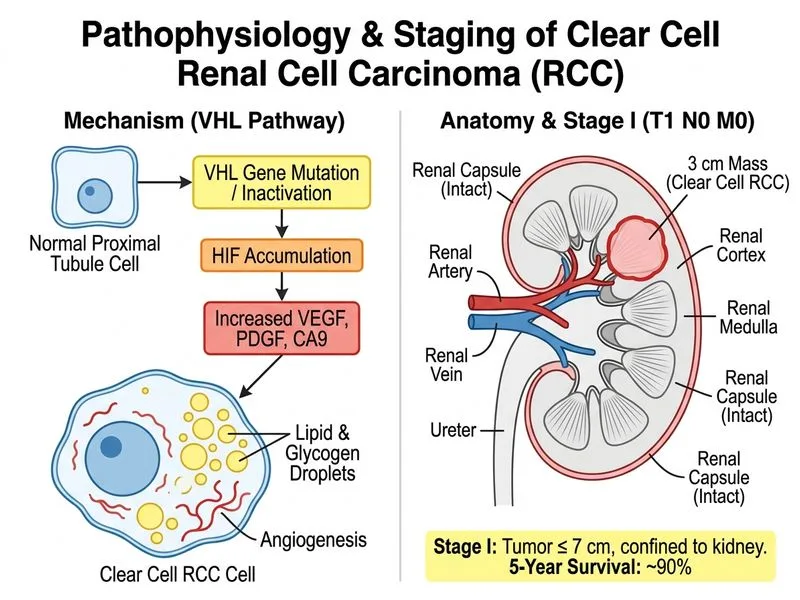
C. Clear cell RCC, Stage I, 5-year survival ~90%
D. Chromophobe RCC, Stage I, 5-year survival ~95%
Explanation
Histopathological Diagnosis
Key Point
The combination of clear cytoplasm, well-defined cell borders, low nuclear grade, and positive CAIX immunostaining is pathognomonic for clear cell RCC. CAIX is highly sensitive and specific for clear cell RCC and is used to confirm the diagnosis when morphology is ambiguous.
Immunohistochemical Profile of RCC Subtypes
Table
Marker
Clear Cell RCC
Papillary RCC
Chromophobe RCC
Oncocytoma
CAIX
✓ Positive
✗ Negative
✗ Negative
✗ Negative
PAX-8
✓ Positive
✓ Positive
✓ Positive
✗ Negative
CK7
✗ Negative
✓ Positive
✗ Negative
✗ Negative
AMACR
✗ Negative
✓ Positive
✗ Negative
✗ Negative
Hale's colloidal iron
✗ Negative
✗ Negative
✓ Positive
✗ Negative
High-YieldNEET PG
CAIX (carbonic anhydrase IX) is the most specific marker for clear cell RCC and reflects HIF-1α activation due to VHL gene inactivation. CK7 negativity excludes papillary RCC, which is typically CK7-positive.
TNM Staging & Prognosis for Stage I Clear Cell RCC
Stage I: Tumor ≤7 cm, confined to kidney (T1, N0, M0)
IA: ≤4 cm
IB: 4–7 cm
Stage II: Tumor >7 cm, confined to kidney (T2, N0, M0)
Stage III: Invasion of renal vein or regional lymph nodes (T3 or N1, M0)
Stage IV: Invasion beyond Gerota's fascia or distant metastases (T4 or M1)
Clinical Pearl
This patient has a Stage IA tumor (3 cm, no invasion, no metastases). The 5-year survival for Stage I clear cell RCC is approximately 90%, reflecting the excellent prognosis when tumors are detected early and confined to the kidney.
Loading diagram...
High-YieldNEET PG
Early detection of small, localized clear cell RCC (Stage I) offers the best prognosis. Partial nephrectomy is the gold standard for tumors ≤4 cm, preserving renal function in CKD patients.
Clinical Context: CKD and RCC Risk
Key Point
Patients with CKD have a 10–20-fold increased risk of RCC compared to the general population. This is thought to be related to chronic uremia, anemia, and use of certain medications (e.g., phenacetin, NSAIDs). Regular screening with ultrasound is recommended in CKD stage 3b–5 patients.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.