A 58-year-old man presents with haematuria and flank pain. Ultrasound shows a 4 cm heterogeneous mass in the right kidney with areas of necrosis. Which investigation is most appropriate for staging and detecting metastases before surgical planning?
A. Contrast-enhanced CT chest, abdomen and pelvis
B. PET-CT with 18F-FDG
C. Renal artery angiography
D. MRI abdomen with gadolinium
Explanation
Investigation of Choice for RCC Staging
Key Point
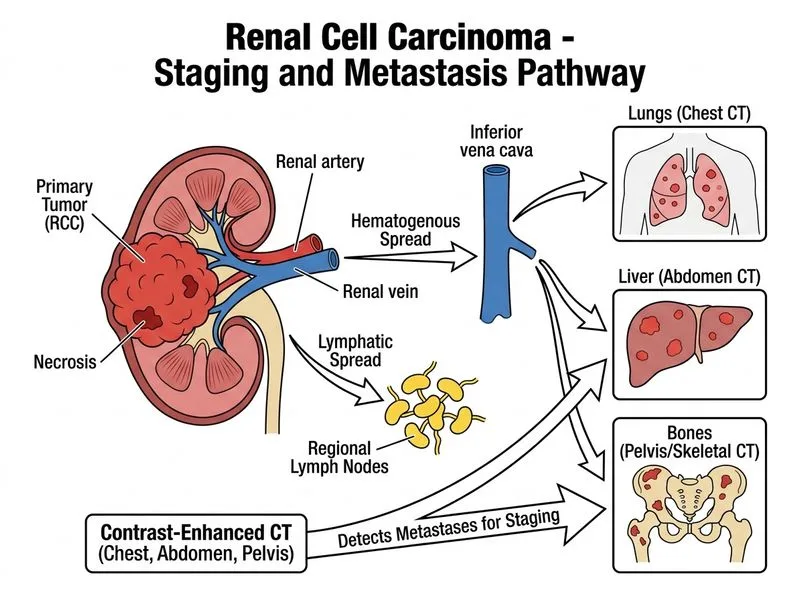
Contrast-enhanced CT (CECT) of chest, abdomen, and pelvis is the gold standard for staging renal cell carcinoma and detecting metastases.
Why CECT is Superior
Table
Feature
CECT
MRI
PET-CT
Angiography
Sensitivity for RCC
95–98%
90–95%
70–80%
N/A (invasive)
Detects renal vein invasion
Excellent
Excellent
Poor
N/A
Lung metastases
Excellent
Limited
Good
N/A
Bone metastases
Good
Good
Excellent
N/A
Liver metastases
Excellent
Excellent
Moderate
N/A
Speed & availability
Fast, widely available
Slower
Limited availability
Invasive
Contraindications
Contrast allergy, renal insufficiency
Pacemaker, claustrophobia
N/A
Invasive, thrombosis risk
High-YieldNEET PG
CECT is the first-line imaging for RCC because it:
1.
Characterizes the renal mass (enhancement pattern, necrosis, calcification)
2.
Assesses local invasion (perinephric fat, renal vein, IVC)