A 52-year-old woman with a history of chronic kidney disease undergoes ultrasound for hypertension workup. A 2.5 cm hyperechoic mass is incidentally found in the left kidney. Ultrasound cannot definitively characterise it as benign or malignant. What is the most appropriate next investigation?
A. Follow-up ultrasound in 3 months
B. MRI abdomen without gadolinium
C. Contrast-enhanced CT of abdomen and pelvis
D. Renal biopsy under ultrasound guidance
Explanation
Characterisation of Indeterminate Renal Mass
Key Point
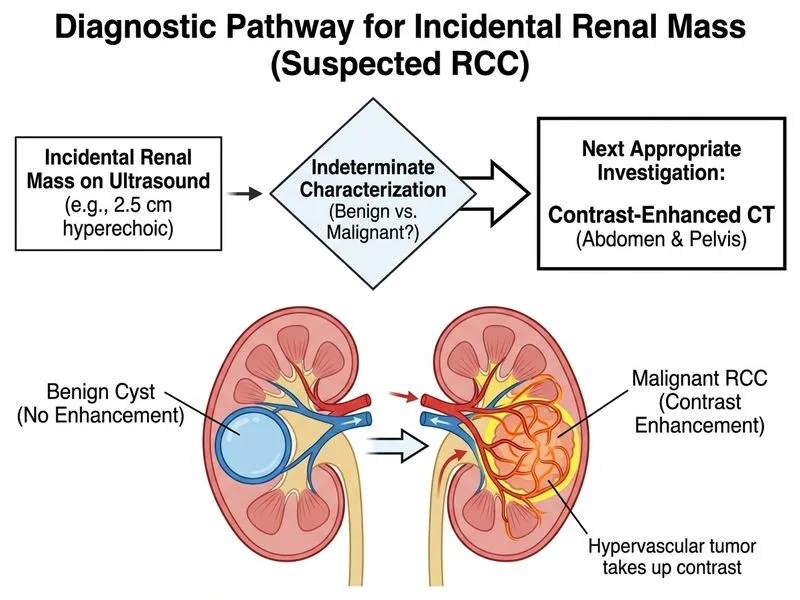
When ultrasound cannot definitively characterise a renal mass as benign or malignant, contrast-enhanced CT (CECT) is the next best investigation because it reliably distinguishes solid tumours from cysts and characterises enhancement patterns.
Diagnostic Algorithm for Indeterminate Renal Mass
Loading diagram...
Why CECT is Superior for Characterisation
Table
Feature
CECT
Renal Biopsy
MRI (no gadolinium)
Follow-up US
Characterises mass
Excellent (enhancement pattern)
Tissue diagnosis but invasive
Limited without contrast
Limited
Detects enhancement
Yes (arterial, venous, delayed)
N/A
No (no gadolinium)
No
Distinguishes RCC from benign
95% sensitivity
100% but invasive
Poor without contrast
Unreliable
Risk of complications
Contrast reaction, nephropathy
Bleeding, infection, seeding
None
Delayed diagnosis
Cost-effective
Yes
Expensive, invasive
Expensive
Delays diagnosis
High-YieldNEET PG
CECT enhancement patterns in renal masses:
RCC: Arterial phase enhancement (>20 HU increase), washout in delayed phase
Oncocytoma: Homogeneous enhancement, central scar (benign)
Angiomyolipoma (AML): Fat density (−10 to −100 HU) on unenhanced CT — diagnostic
Simple cyst: No enhancement, water density (0–20 HU)
Invasive with risk of bleeding, infection, and tumour seeding
Reserved for:
Confirmation of diagnosis when imaging is equivocal AND management depends on it
Suspected metastatic disease to kidney
Evaluation of renal dysfunction (not applicable here)
NOT first-line for characterising an indeterminate mass
MRI without gadolinium:
Gadolinium is essential for characterising renal masses (contrast-enhanced MRI = CEMRI)
Non-contrast MRI provides no enhancement information and cannot reliably distinguish RCC from benign lesions
Delays diagnosis unnecessarily
Follow-up ultrasound in 3 months:
Ultrasound has poor specificity for characterising solid renal masses
Delays diagnosis of potentially malignant lesion
If mass is RCC, delay increases stage and reduces survival
Only appropriate for clearly benign cysts (Bosniak I) or in patients with contraindications to contrast
Clinical Pearl
A 2.5 cm hyperechoic mass on ultrasound is suspicious for RCC (clear cell carcinoma often appears hyperechoic due to lipid content) or benign lesions (oncocytoma, AML). CECT will definitively characterise it:
If it enhances in arterial phase → likely RCC → proceed to staging and surgery
If it shows fat density → AML (benign) → conservative management
If it shows no enhancement → likely oncocytoma → follow-up imaging
Mnemonic: CECT for indeterminate mass = Characterise, Enhancement pattern, Confirm diagnosis, Treatment planning.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.