A 58-year-old man from Delhi presents with a 3-month history of flank pain, haematuria, and constitutional symptoms (weight loss 4 kg, low-grade fever). On examination, he is pale and has a palpable left flank mass. Contrast-enhanced CT abdomen shows a 6 cm heterogeneous mass in the left kidney with fat stranding and no distant metastases. Chest X-ray and brain MRI are normal. Baseline renal function is normal (creatinine 0.9 mg/dL). What is the most appropriate next step in management?
A. Percutaneous renal biopsy followed by staging
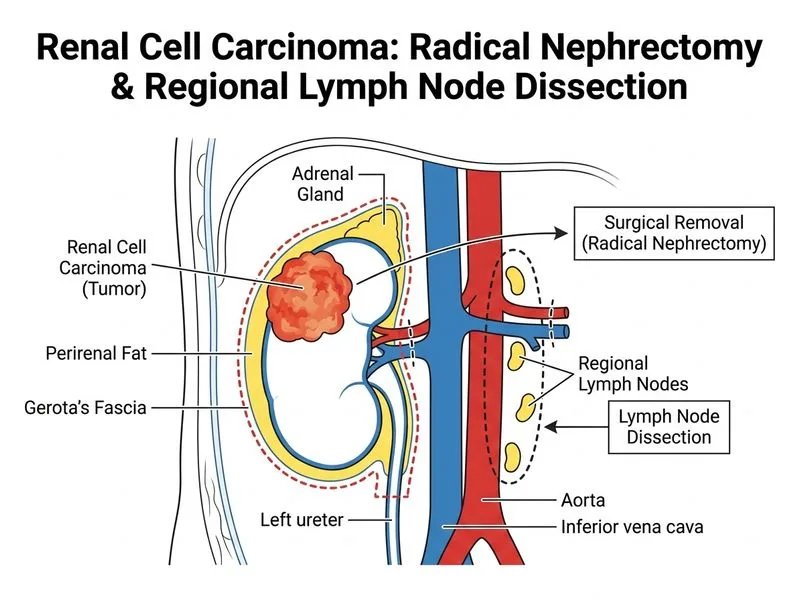
B. Radical nephrectomy with regional lymph node dissection
C. Neoadjuvant targeted therapy (sunitinib) for 3 months, then reassess
D. Palliative chemotherapy with gemcitabine and cisplatin
Explanation
Clinical Context
This patient has a localized renal cell carcinoma (RCC) with no evidence of metastatic disease. The imaging findings (6 cm mass, fat stranding) and clinical presentation are classic for RCC. The absence of distant metastases and normal renal function make him a candidate for curative surgical resection.
Management Algorithm for Localized RCC
Loading diagram...
Why Radical Nephrectomy is Correct
Key Point
For localized RCC (Stage I–III, no metastases), radical nephrectomy with regional lymph node dissection is the gold standard curative treatment.
High-YieldNEET PG
Radical nephrectomy removes the kidney, perirenal fat, Gerota's fascia, and ipsilateral adrenal gland (if involved).
Regional lymph node dissection improves staging accuracy and may confer survival benefit in node-positive disease.
This patient has no contraindications: normal contralateral kidney function, no distant metastases, and fit for surgery.
Clinical Pearl
The presence of constitutional symptoms (fever, weight loss) and haematuria does not change the management of localized disease — these are paraneoplastic manifestations and will resolve post-nephrectomy if disease is completely resected.
Adjuvant Considerations
Table
Feature
Implication
6 cm mass
T2 (intermediate risk)
No necrosis/sarcomatoid noted
Standard risk
No nodal involvement (on imaging)
N0
No metastases
M0
Stage: II–III
Candidate for adjuvant therapy if high-risk features confirmed on pathology
Tip
Post-operative pathology may reveal high-risk features (Fuhrman grade 3–4, sarcomatoid, necrosis) → adjuvant sunitinib or pazopanib is then considered. But surgery is the immediate next step.
Robbins 10e Ch 20
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.