This is a small, localized renal mass (2.8 cm, Stage T1a) with no metastatic disease. The patient is young, fit, and has normal renal function. The key decision is between nephron-sparing surgery (partial nephrectomy), ablation, and surveillance.
| Approach | Indication | Pros | Cons | Oncologic Outcome |
|---|---|---|---|---|
| Partial nephrectomy | T1a, normal bilateral kidneys, fit patient | Preserves renal function, excellent cancer control | Technically demanding, longer operative time | 5-yr DFS >95% |
| Radical nephrectomy | T1a with solitary kidney contraindication or patient refusal | Simpler surgery, complete tumour removal | Unnecessary renal loss in fit patients | 5-yr DFS >95% |
| Ablation (RFA/cryo) | T1a, elderly/unfit, poor surgical candidate | Minimally invasive, outpatient | Higher recurrence in large T1a, less data | 5-yr local control ~90% |
| Surveillance | T1a, very elderly, limited life expectancy | Avoids surgery | Risk of delayed diagnosis, tumour growth | Variable, not recommended for fit patients |
Robbins 10e Ch 20; NCCN Kidney Cancer Guidelines 2023
Loading illustration…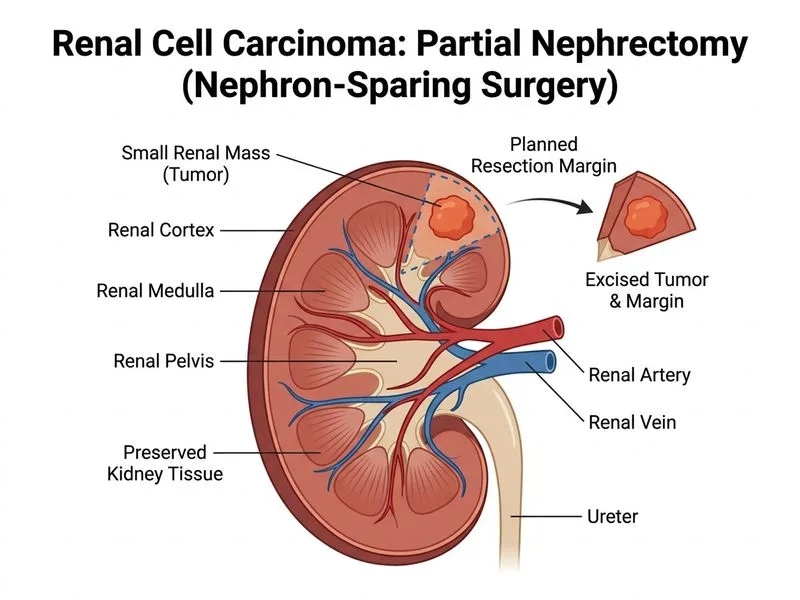
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →