A 28-week gestation male infant is delivered via emergency cesarean section for placental abruption. Birth weight 1.2 kg. At 2 hours of life, the infant develops grunting, nasal flaring, and intercostal retractions. Oxygen saturation drops to 88% on room air. Chest X-ray shows a fine reticular granular pattern with air bronchograms and a ground-glass appearance. What is the most likely diagnosis?
A. Transient Tachypnea of the Newborn
B. Respiratory Distress Syndrome (Hyaline Membrane Disease)
C. Meconium Aspiration Syndrome
D. Congenital Pneumonia
Explanation
Clinical Presentation & Diagnosis
Key Point
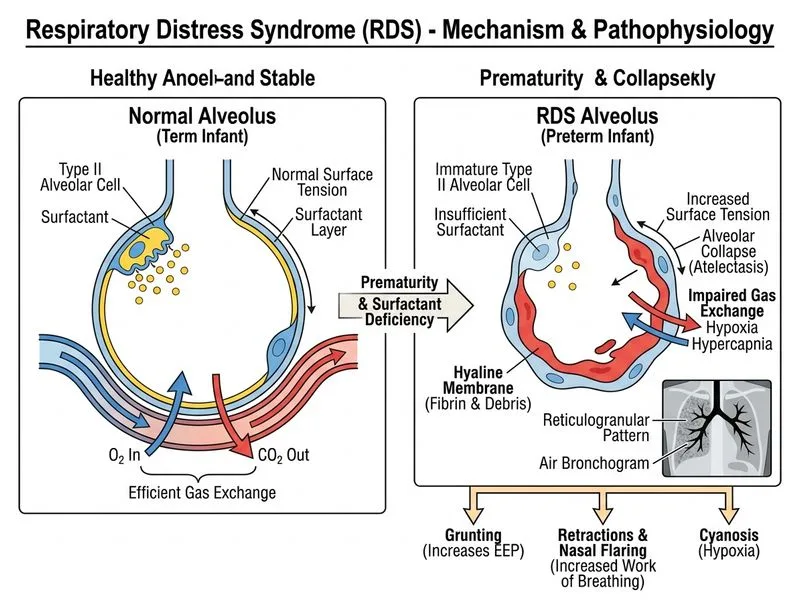
Respiratory Distress Syndrome (RDS), also called Hyaline Membrane Disease (HMD), is the most common cause of respiratory distress in preterm infants and is caused by surfactant deficiency.
Why This Case Fits RDS
1.
Gestational age: 28 weeks is in the highest-risk window (22–32 weeks). Surfactant production begins at ~24 weeks but is insufficient until 34–36 weeks.
2.
Timing of onset: Symptoms within the first 2 hours of life are classic for RDS; other conditions (TTN, meconium aspiration) typically present later or have different triggers.
3.
Clinical signs: Grunting (attempt to maintain positive end-expiratory pressure), nasal flaring, intercostal retractions, and hypoxemia are hallmark features.
4.
Chest X-ray findings: The fine reticular granular pattern with air bronchograms and ground-glass appearance is pathognomonic for HMD. This represents atelectasis alternating with hyperinflated alveoli due to uneven ventilation from surfactant deficiency.
Pathophysiology
High-YieldNEET PG
Surfactant (a lipoprotein complex rich in phospholipids, especially dipalmitoylphosphatidylcholine [DPPC]) reduces surface tension in alveoli. Without it, alveoli collapse at end-expiration (atelectasis), requiring enormous pressure to re-expand them with each breath — leading to work of breathing, fatigue, and hypoxemia.
Risk Factors for RDS
Table
Factor
Impact
Prematurity (< 34 weeks)
Highest risk; surfactant immature
Male sex
1.5–2× higher risk than females
Maternal diabetes
Delays fetal lung maturity
Cesarean delivery (especially elective, without labor)
No thoracic compression to expel fetal lung fluid
Perinatal asphyxia
Reduces surfactant synthesis
Maternal hemorrhage / placental insufficiency
Fetal stress impairs maturation
Management Principles
Loading diagram...
Clinical Pearl
Antenatal corticosteroids (betamethasone or dexamethasone) given to the mother 24 hours to 7 days before preterm delivery significantly reduce RDS incidence and severity by accelerating fetal lung maturation.
Mnemonic: SURFACTANT — Surface tension reduction, Uneven ventilation (atelectasis), Reticular granular pattern (CXR), Fetal immaturity, Air bronchograms, Classic in preterm, Timing early (first hours), Antepartum steroids prevent, Need exogenous replacement, Tachypnea & grunting.
High-YieldNEET PG
Exogenous surfactant (e.g., beractant, poractant alfa) given via endotracheal tube within the first hours of life is the definitive treatment and dramatically improves survival and reduces chronic lung disease.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.