A 28-week gestation male infant born to a mother with rupture of membranes 6 hours prior presents with grunting, intercostal retractions, and nasal flaring within 2 hours of birth. Chest X-ray shows a ground-glass appearance with air bronchograms. Arterial blood gas shows pH 7.28, PaCO₂ 52 mmHg, PaO₂ 48 mmHg on room air. What is the most appropriate immediate next step in management?
A. Perform immediate intubation and mechanical ventilation without surfactant
B. Administer antenatal corticosteroids and observe for spontaneous improvement
C. Start high-flow nasal cannula oxygen and defer further intervention pending response
D. Initiate continuous positive airway pressure (CPAP) and administer exogenous surfactant
Explanation
Clinical Diagnosis
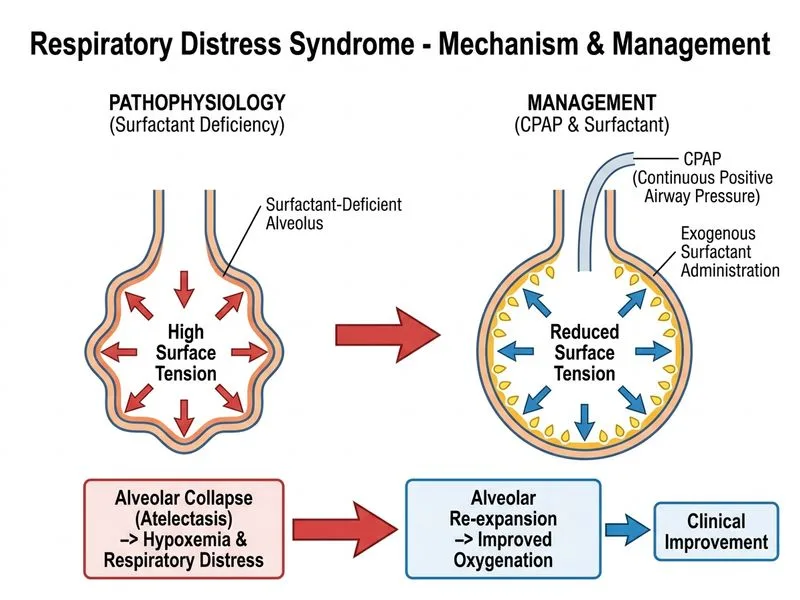
This is a classic presentation of Respiratory Distress Syndrome (RDS) in a preterm infant (28 weeks gestation). The clinical triad of grunting, retractions, and nasal flaring, combined with ground-glass opacification on chest X-ray and hypoxemia with hypercapnia, confirms RDS due to surfactant deficiency.
Pathophysiology of RDS
Surfactant production begins around 24 weeks gestation but is inadequate until ~34–35 weeks. Without surfactant:
Compliance decreases → increased work of breathing
Ventilation–perfusion mismatch → hypoxemia and hypercapnia
Management Algorithm
Loading diagram...
Why CPAP + Surfactant is Correct
Key Point
CPAP (Continuous Positive Airway Pressure) is the first-line non-invasive respiratory support for RDS in preterm infants. It:
Maintains positive end-expiratory pressure (PEEP) to prevent alveolar collapse
Reduces work of breathing
Allows spontaneous breathing
Minimizes ventilator-induced lung injury (VILI)
High-YieldNEET PG
Exogenous surfactant replacement is the definitive treatment for RDS. Modern approach is "INSURE" (Intubate–Surfactant–Extubate) or "CPAP-first" strategy:
Administer surfactant via thin endotracheal tube or laryngeal mask airway
Extubate immediately back to CPAP if possible
This reduces need for prolonged mechanical ventilation and decreases BPD risk
Clinical Pearl
In this case, the infant has moderate-to-severe RDS (PaO₂ 48 mmHg on room air, pH 7.28). CPAP alone may not be sufficient; surfactant administration is indicated. The combination of CPAP + surfactant is the standard of care and offers the best balance of efficacy and lung protection.
Why Other Options Are Suboptimal
Table
Option
Why Wrong
Antenatal corticosteroids + observation
Antenatal steroids accelerate fetal lung maturity but are given before delivery; they cannot be given now. Observation alone will lead to progressive hypoxemia and respiratory failure.
Immediate intubation without surfactant
Intubation without surfactant leaves the underlying deficiency untreated. Mechanical ventilation alone increases VILI risk and BPD.
High-flow nasal cannula + defer intervention
High-flow nasal cannula provides insufficient support for this degree of RDS. Deferring surfactant allows progressive atelectasis and deterioration.
Warning
Do not confuse CPAP-first strategy with "no surfactant." CPAP is the respiratory support modality; surfactant is the pharmacological treatment. Both are needed in moderate-to-severe RDS.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.