A 34-week gestation female infant delivered via emergency cesarean section for fetal distress is now 4 hours old. She has mild tachypnea (respiratory rate 58/min), minimal intercostal retractions, and oxygen saturation of 92% on room air. Chest X-ray shows mild hyperinflation with some areas of atelectasis. Blood gas is normal. The infant is feeding well and maintaining temperature. What is the most appropriate next step?
A. Administer a single dose of surfactant immediately to prevent deterioration
B. Observe closely with continuous pulse oximetry; provide supportive care and reassess in 2–4 hours
C. Initiate mechanical ventilation to prevent complications of RDS
D. Start CPAP prophylactically to prevent progression to severe RDS
Explanation
Clinical Presentation: Mild RDS or Transient Tachypnea?
This constellation suggests either mild RDS or transient tachypnea of the newborn (TTN), both of which often resolve spontaneously with supportive care.
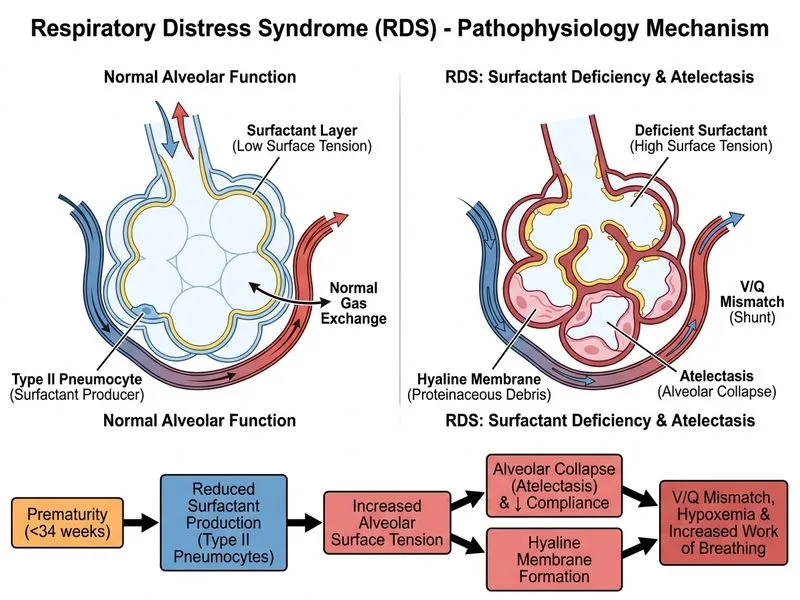
Pathophysiology: Why Observation Is Safe Here
Key Point
Not all preterm infants with mild respiratory symptoms require immediate pharmacological or invasive intervention. The natural history of mild RDS in late preterm infants (34 weeks) is often self-limited:
Endogenous surfactant production is increasing at 34 weeks (though not yet mature)
Lung compliance improves over the first 12–24 hours
Many infants improve with oxygen supplementation and PEEP alone (via nasal cannula or observation)
High-YieldNEET PG
The "watch-and-wait" approach with close monitoring is evidence-based for mild RDS:
Reduces unnecessary interventions and associated morbidity
Avoids surfactant administration in infants who may not need it
Maintain normothermia, normal glucose, and adequate hydration
Encourage feeding if infant is stable
Reassess in 2–4 hours; escalate support if deterioration occurs
Clinical Pearl
Late preterm infants (34–36 weeks) have significantly better outcomes than earlier preterm infants. Many require only observation and supplemental oxygen, not CPAP or surfactant. Escalate care only if clinical deterioration occurs.
Why Other Options Are Premature
Table
Option
Why Wrong
Prophylactic CPAP
CPAP is indicated for moderate-to-severe RDS or if the infant deteriorates. Applying CPAP to every mildly tachypneic infant increases unnecessary intervention and risk of barotrauma.
Prophylactic surfactant
Surfactant is indicated for confirmed or worsening RDS, not for mild symptoms in a stable infant with normal blood gas. Unnecessary surfactant increases cost and infection risk.
Immediate mechanical ventilation
Intubation is reserved for severe RDS with respiratory failure. This infant is oxygenating adequately and has normal ventilation.
Warning
Do not over-treat mild RDS. The goal is to provide the least invasive support that maintains adequate oxygenation and ventilation. Many infants improve spontaneously with oxygen and observation alone.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.