A 28-year-old woman from rural Maharashtra presents with progressive dyspnea on exertion for 6 months and orthopnea. She has a history of recurrent sore throat in childhood. On examination, she has an irregular pulse (90–110 bpm), a loud S1, an opening snap at the apex, and a low-pitched diastolic murmur best heard at the apex in the left lateral decubitus position. Chest X-ray shows straightening of the left heart border and pulmonary congestion. Echocardiography reveals a thickened, domed mitral valve with restricted leaflet motion and a valve area of 1.2 cm². What is the most likely diagnosis?
A. Constrictive pericarditis
B. Acute rheumatic fever with carditis
C. Mitral stenosis secondary to rheumatic heart disease
Mitral regurgitation secondary to rheumatic heart disease
The combination of history of recurrent sore throat, loud S1, opening snap, low-pitched diastolic murmur (Carey Coombs murmur), and echocardiographic findings of a thickened, domed mitral valve with restricted leaflet motion and reduced valve area (1.2 cm²) is pathognomonic for mitral stenosis (MS) secondary to rheumatic heart disease (RHD).
Pathophysiology of Rheumatic Mitral Stenosis
1.
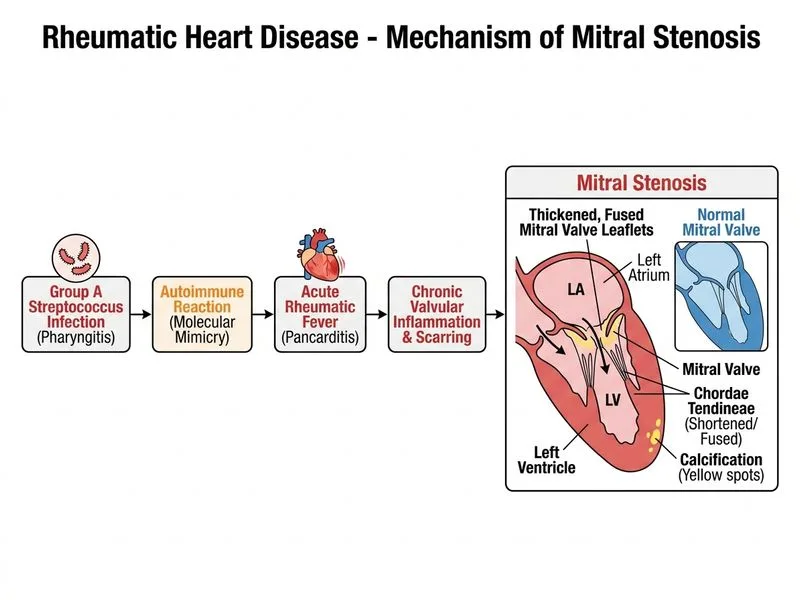
Post-streptococcal autoimmune reaction → molecular mimicry between Group A Streptococcus (GAS) M-protein and cardiac myosin
2.
Acute rheumatic fever (ARF) → pancarditis with valve inflammation
3.
Chronic phase → fibrosis, calcification, and commissural fusion of mitral leaflets
4.
Result: Progressive narrowing of the mitral orifice, increased left atrial pressure, and pulmonary congestion
Diagnostic Hallmarks of Mitral Stenosis
Table
Feature
Significance
Loud S1
Increased force of valve closure due to elevated LA pressure
Opening snap
Abrupt halting of domed leaflet motion in early diastole
Diastolic murmur
Low-pitched, rumbling, best at apex in left lateral decubitus
Irregular pulse
Atrial fibrillation (common in chronic MS due to LA enlargement)
Straightening of left heart border
LA enlargement on CXR
Valve area < 1.5 cm²
Moderate-to-severe stenosis; normal = 4–6 cm²
Clinical Pearl
The opening snap occurs earlier in diastole when MS is more severe (higher LA pressure pushes leaflets open faster). The A2–OS interval shortens as severity increases.
Echocardiographic Criteria for RHD Mitral Stenosis
High-YieldNEET PG
Echocardiography is the gold standard for diagnosis and severity assessment:
Thickened leaflets (>3 mm) with restricted motion
Domed anterior leaflet in systole (characteristic of RHD)
This patient's valve area of 1.2 cm² indicates moderate stenosis.
Why This Is RHD and Not Acute Rheumatic Fever
Key Point
This patient has chronic, established mitral stenosis, not acute carditis. ARF presents acutely with pancarditis (endocarditis, myocarditis, pericarditis), new or changing murmurs, and systemic features (fever, arthritis, chorea, erythema marginatum, subcutaneous nodules). This patient has a 6-month history of progressive dyspnea with structural valve changes — classic for chronic RHD.
Management Implications
Medical: Diuretics, beta-blockers (rate control), anticoagulation if AF present
Interventional: Percutaneous mitral balloon commissurotomy (PMBC) if valve area 1.0–1.5 cm² and favorable anatomy
Surgical: Mitral valve replacement if severe stenosis, unfavorable anatomy, or failed PMBC
Mnemonic for RHD sequelae: MAST
Mitral stenosis (most common, ~65%)
Aortic regurgitation (second most common)
Stenosis of aortic valve
Tricuspid involvement (least common)
Robbins 10e Ch 12
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.