A 35-year-old man with a history of acute rheumatic fever (ARF) 15 years ago presents with palpitations and dyspnea. Echocardiography shows moderate aortic regurgitation (AR) with a regurgitant jet width of 8 mm and aortic root diameter of 50 mm. Left ventricular ejection fraction (LVEF) is 50%. He is currently on no cardiac medications. What is the most appropriate next step in management?
A. Start beta-blocker monotherapy and observe with annual echocardiography
B. Refer for aortic valve replacement immediately
C. Start amlodipine and lisinopril; repeat echocardiography in 6 months
D. Perform cardiac catheterization to assess hemodynamic severity
Explanation
Clinical Context
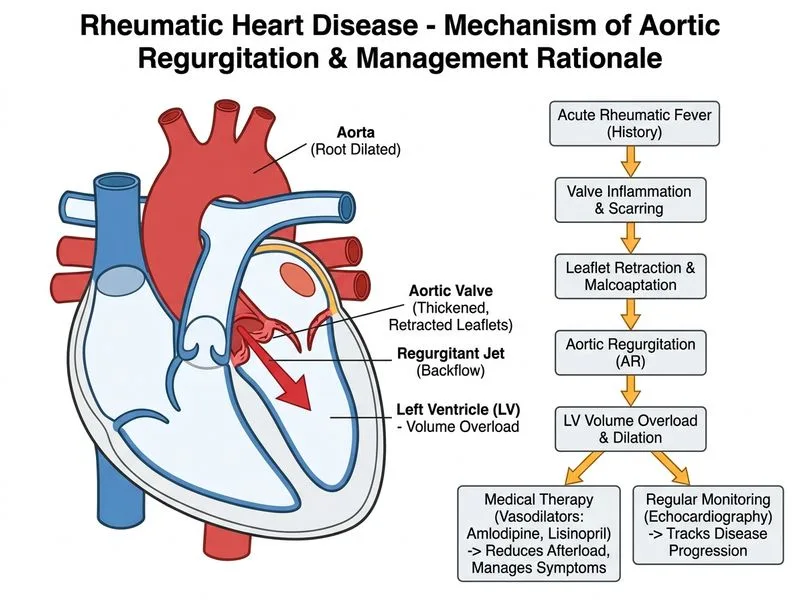
This patient has chronic aortic regurgitation (AR) secondary to rheumatic heart disease presenting with symptoms (palpitations and dyspnea), an aortic root diameter of 50 mm, and a borderline-reduced LVEF of 50%. The combination of these findings meets guideline-based indications for aortic valve replacement (AVR).
Classification of Aortic Regurgitation Severity
Table
Parameter
Mild
Moderate
Severe
Jet width (% LVOT)
<25%
25–65%
>65%
Regurgitant volume (mL/beat)
<30
30–59
≥60
Aortic root diameter
<40 mm
40–50 mm
≥50 mm
LVEF
Normal
Normal–mildly ↓
↓
Key Point
An aortic root diameter of ≥50 mm is classified as severe dilatation per ACC/AHA 2021 and ESC 2021 guidelines, and in a symptomatic patient with LVEF at 50% (borderline impaired in the context of chronic volume overload), this constitutes a clear surgical indication.
Indications for Aortic Valve Replacement in AR (ACC/AHA 2021 / ESC 2021)
High-YieldNEET PG
Surgery is indicated when ANY of the following are present:
1.
Symptomatic severe AR (dyspnea, angina, syncope) — Class I
2.
Asymptomatic severe AR with LVEF ≤55% (ACC/AHA) or LVEF <50% (ESC) — Class I
3.
Aortic root/ascending aorta ≥50 mm in patients with bicuspid valve or connective tissue disease, or ≥55 mm in others — Class I
4.
Severe AR undergoing other cardiac surgery — Class I
This patient is symptomatic (dyspnea, palpitations) AND has LVEF of 50% (below the ACC/AHA threshold of 55% and at the ESC threshold of <50%), AND has an aortic root of 50 mm — meeting multiple Class I indications simultaneously.
Why Immediate AVR is Correct
1.
Symptomatic status: Dyspnea and palpitations in the setting of AR indicate hemodynamic compromise — medical therapy alone is insufficient.
2.
LVEF 50%: In chronic AR, the LV compensates with eccentric hypertrophy; an LVEF of 50% represents significant myocardial impairment (normal compensation should maintain LVEF >60%). This is a Class I indication for surgery per ACC/AHA 2021 (LVEF ≤55%).
3.
Aortic root 50 mm: At or above the threshold for surgical intervention, particularly in a symptomatic patient.
4.
Delaying surgery risks irreversible LV dysfunction: Once LVEF falls further, post-operative LV recovery is compromised.
Why Other Options Are Incorrect
Option A (Amlodipine + Lisinopril, echo in 6 months): Vasodilators are appropriate for asymptomatic patients with preserved LV function who do not yet meet surgical criteria. This patient is symptomatic with borderline LVEF — delaying surgery with medical therapy risks irreversible LV damage.
Option C (Cardiac catheterization): Echocardiography is sufficient to assess AR severity; catheterization is not routinely required before AVR unless coronary artery disease is suspected (not indicated here as first step).
Option D (Beta-blocker monotherapy): Beta-blockers are contraindicated in chronic AR — they prolong diastole, increase diastolic runoff time, and worsen regurgitant volume. This is a dangerous choice.
Management Algorithm for Chronic AR
Clinical Pearl
In chronic AR, LVEF is a critical decision point. Because the LV dilates to compensate, an LVEF of 50% in AR is equivalent to significant systolic dysfunction — do not be falsely reassured by a "preserved" LVEF that is actually below the expected compensatory range.
Reference: ACC/AHA 2021 Valvular Heart Disease Guidelines (Otto CM et al., JACC 2021); ESC/EACTS 2021 Guidelines on Valvular Heart Disease (Vahanian A et al., Eur Heart J 2022).
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.